

Estradiol increases cortical and trabecular bone accrual and bone strength in an adolescent male-to-female mouse model of gender-affirming hormone therapy
- PMID: 38212599
- PMCID: PMC10784310
- DOI: 10.1038/s41413-023-00308-2
Estradiol increases cortical and trabecular bone accrual and bone strength in an adolescent male-to-female mouse model of gender-affirming hormone therapy
Abstract
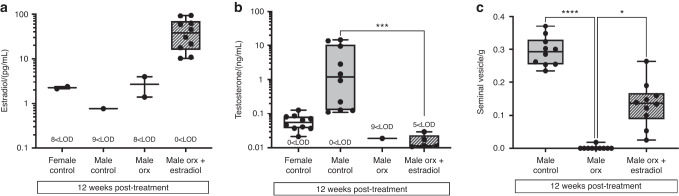
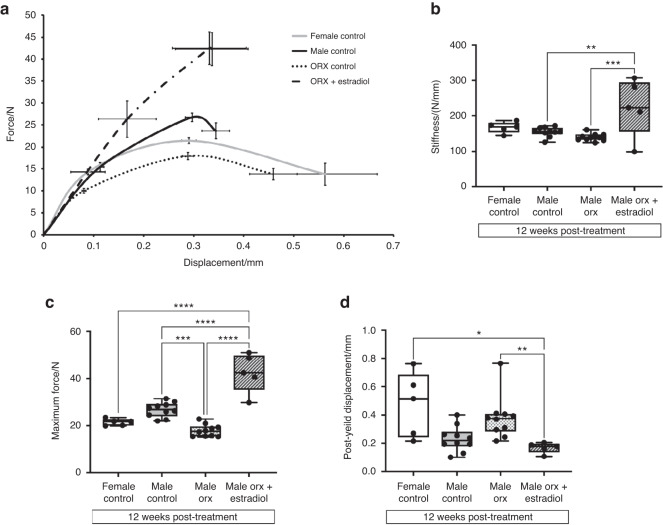
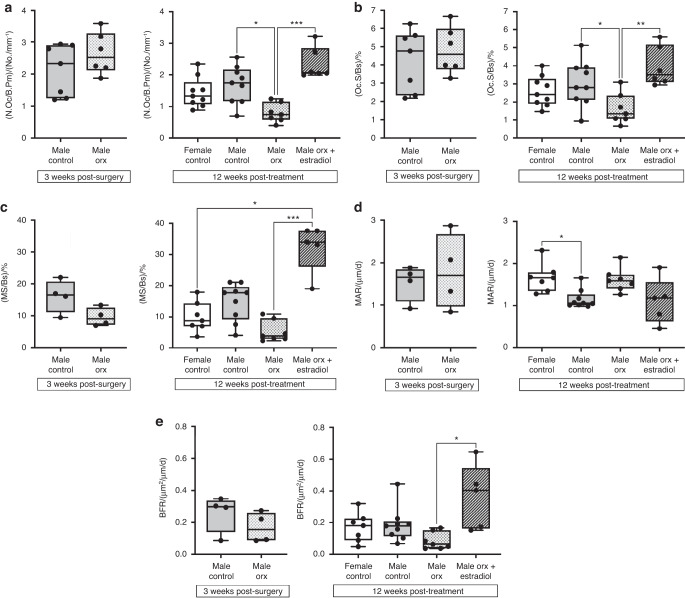
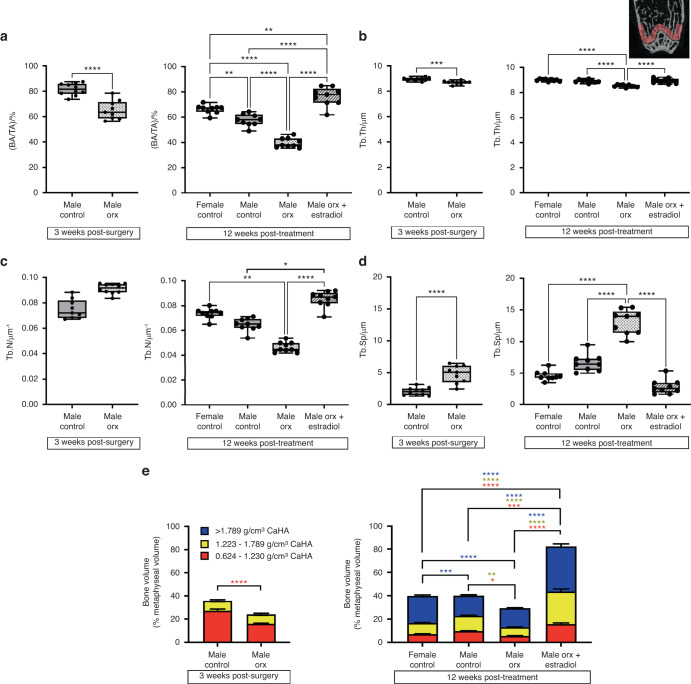
The effects of gender-affirming hormone therapy on the skeletal integrity and fracture risk in transitioning adolescent trans girls are unknown. To address this knowledge gap, we developed a mouse model to simulate male-to-female transition in human adolescents in whom puberty is first arrested by using gonadotrophin-releasing hormone analogs with subsequent estradiol treatment. Puberty was suppressed by orchidectomy in male mice at 5 weeks of age. At 3 weeks post-surgery, male-to-female mice were treated with a high dose of estradiol (~0.85 mg) by intraperitoneal silastic implantation for 12 weeks. Controls included intact and orchidectomized males at 3 weeks post-surgery, vehicle-treated intact males, intact females and orchidectomized males at 12 weeks post-treatment. Compared to male controls, orchidectomized males exhibited decreased peak bone mass accrual and a decreased maximal force the bone could withstand prior to fracture. Estradiol treatment in orchidectomized male-to-female mice compared to mice in all control groups was associated with an increased cortical thickness in the mid-diaphysis, while the periosteal circumference increased to a level that was intermediate between intact male and female controls, resulting in increased maximal force and stiffness. In trabecular bone, estradiol treatment increased newly formed trabeculae arising from the growth plate as well as mineralizing surface/bone surface and bone formation rate, consistent with the anabolic action of estradiol on osteoblast proliferation. These data support the concept that skeletal integrity can be preserved and that long-term fractures may be prevented in trans girls treated with GnRHa and a sufficiently high dose of GAHT. Further study is needed to identify an optimal dose of estradiol that protects the bone without adverse side effects.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
High circulating concentrations of estradiol are anabolic for bone mass and strength in an adult male to female transgender mouse model.Bone. 2024 Sep;186:117143. doi: 10.1016/j.bone.2024.117143. Epub 2024 Jun 10. Bone. 2024. PMID: 38866125
-
Relative impact of androgen and estrogen receptor activation in the effects of androgens on trabecular and cortical bone in growing male mice: a study in the androgen receptor knockout mouse model.J Bone Miner Res. 2006 Apr;21(4):576-85. doi: 10.1359/jbmr.060103. Epub 2006 Apr 5. J Bone Miner Res. 2006. PMID: 16598378
-
Bone quality following peripubertal growth in a mouse model of transmasculine gender-affirming hormone therapy.bioRxiv [Preprint]. 2024 Jan 14:2023.12.08.570840. doi: 10.1101/2023.12.08.570840. bioRxiv. 2024. PMID: 38106067 Free PMC article. Preprint.
-
Unresolved issues in osteoporosis in men.Rev Endocr Metab Disord. 2001 Jan;2(1):45-64. doi: 10.1023/a:1010054924085. Rev Endocr Metab Disord. 2001. PMID: 11704979 Review.
-
Gonadal suppressive and cross-sex hormone therapy for gender dysphoria in adolescents and adults.Pharmacotherapy. 2014 Dec;34(12):1282-97. doi: 10.1002/phar.1487. Epub 2014 Sep 15. Pharmacotherapy. 2014. PMID: 25220381 Review.
Cited by
-
Sexual Dimorphism in the Musculoskeletal System: Sex Hormones and Beyond.J Endocr Soc. 2024 Sep 1;8(10):bvae153. doi: 10.1210/jendso/bvae153. eCollection 2024 Aug 27. J Endocr Soc. 2024. PMID: 39309123 Free PMC article. Review.
-
Antioxidant 1,2,3,4,6-Penta-O-galloyl-β-D-glucose Alleviating Apoptosis and Promoting Bone Formation Is Associated with Estrogen Receptors.Molecules. 2024 Oct 29;29(21):5110. doi: 10.3390/molecules29215110. Molecules. 2024. PMID: 39519751 Free PMC article.
-
Serum Uric Acid and Bone Health in Middle-Aged and Elderly Hypertensive Patients: A Potential U-Shaped Association and Implications for Future Fracture Risk.Metabolites. 2025 Jan 3;15(1):15. doi: 10.3390/metabo15010015. Metabolites. 2025. PMID: 39852358 Free PMC article.
-
Therapeutic Efficacy of Medicinal Plants with Allopathic Medicine in Musculoskeletal Diseases.Int J Plant Anim Environ Sci. 2024;14(4):104-129. doi: 10.26502/ijpaes.4490170. Epub 2024 Dec 23. Int J Plant Anim Environ Sci. 2024. PMID: 39866300 Free PMC article.
-
Inverted U-shaped association between total testosterone with bone mineral density in men over 60 years old.BMC Endocr Disord. 2024 Nov 18;24(1):249. doi: 10.1186/s12902-024-01780-5. BMC Endocr Disord. 2024. PMID: 39558326 Free PMC article.
References
-
- Klink D, Caris M, Heijboer A, van Trotsenburg M, Rotteveel J. Bone mass in young adulthood following gonadotropin-releasing hormone analog treatment and cross-sex hormone treatment in adolescents with gender dysphoria. J. Clin. Endocrinol. Metab. 2015;100:E270–E275. doi: 10.1210/jc.2014-2439. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
