

Risk factors for recognized and unrecognized SARS-CoV-2 infection: a seroepidemiologic analysis of the Prospective Urban Rural Epidemiology (PURE) study
- PMID: 38214526
- PMCID: PMC10845948
- DOI: 10.1128/spectrum.01492-23
Risk factors for recognized and unrecognized SARS-CoV-2 infection: a seroepidemiologic analysis of the Prospective Urban Rural Epidemiology (PURE) study
Abstract
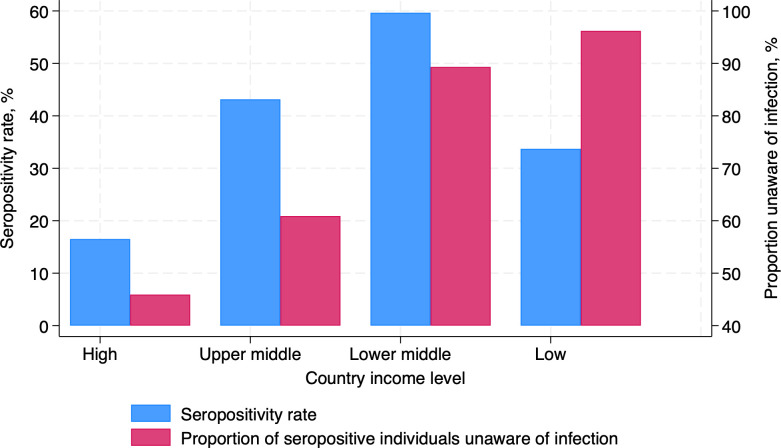
There are limited data on individual risk factors for SARS-CoV-2 infection (including unrecognized infection). In this seroepidemiologic substudy of an ongoing prospective cohort study of community-dwelling adults, participants were thoroughly characterized pre-pandemic. The SARS-CoV-2 infection was ascertained by serology. Among 8,719 participants from 11 high-, middle-, and low-income countries, 3,009 (35%) were seropositive for SARS-CoV-2. Characteristics independently associated with seropositivity were younger age (odds ratio, OR; 95% confidence interval, CI, per five-year increase: 0.95; 0.91-0.98) and body mass index >25 kg/m2 (OR, 95% CI: 1.16, 1.01-1.34). Smoking (as compared with never smoking, OR, 95% CI: 0.83, 0.70-0.97) and COVID-19 vaccination (OR, 95% CI: 0.70, 0.60-0.82) were associated with a reduced risk of seropositivity. Among seropositive participants, 83% were unaware of having been infected with SARS-CoV-2. Seropositivity and a lack of awareness of infection were more common in lower-income countries. The COVID-19 vaccination reduces the risk of SARS-CoV-2 infection (including recognized and unrecognized infections). Overweight or obesity is an independent risk factor for SARS-CoV-2 infection. Infection and lack of infection awareness are more common in lower-income countries.IMPORTANCEIn this large, international study, evidence of SARS-CoV-2 infection was obtained by testing blood specimens from 8,719 community-dwelling adults from 11 countries. The key findings are that (i) the large majority (83%) of community-dwelling adults from several high-, middle-, and low-income countries with blood test evidence of SARS-CoV-2 infection were unaware of this infection-especially in lower-income countries; and (ii) overweight/obesity predisposes to SARS-CoV-2 infection, while COVID-19 vaccination is associated with a reduced risk of SARS-CoV-2 infection. These observations are not attributable to other individual characteristics, highlighting the importance of the COVID-19 vaccination to prevent not only severe infection but possibly any infection. Further research is needed to understand the mechanisms by which overweight/obesity might increase the risk of SARS-CoV-2 infection.
Keywords: COVID-19; SARS-CoV-2; low-income countries; pandemic; seroepidemiology; transmission.
Conflict of interest statement
M.L.D. has served on vaccine advisory boards for GSK, Sanofi, Pfizer, Janssen, Novavax, Medicago, Seqirus, and Merck and on Data Safety Monitoring Boards for CanSino Biologic and has received in-kind vaccine from Sanofi and funding from the World Health Organization, the Canadian Institutes of Health Research, and the Medical Research Council UK.
Figures
Similar articles
-
Seroprevalence of SARS-CoV-2 infection and associated factors among Bangladeshi slum and non-slum dwellers in pre-COVID-19 vaccination era: October 2020 to February 2021.PLoS One. 2022 May 23;17(5):e0268093. doi: 10.1371/journal.pone.0268093. eCollection 2022. PLoS One. 2022. PMID: 35604947 Free PMC article.
-
Pre-Vaccine Positivity of SARS-CoV-2 Antibodies in Alberta, Canada during the First Two Waves of the COVID-19 Pandemic.Microbiol Spectr. 2021 Sep 3;9(1):e0029121. doi: 10.1128/Spectrum.00291-21. Epub 2021 Aug 18. Microbiol Spectr. 2021. PMID: 34406813 Free PMC article.
-
Seroprevalence of SARS-CoV-2 specific Immunoglobin G antibodies in rural population of Western Maharashtra, India.J Glob Health. 2023 Apr 21;13:06011. doi: 10.7189/jogh.13.06011. J Glob Health. 2023. PMID: 37079274 Free PMC article.
-
Universal screening for SARS-CoV-2 infection: a rapid review.Cochrane Database Syst Rev. 2020 Sep 15;9(9):CD013718. doi: 10.1002/14651858.CD013718. Cochrane Database Syst Rev. 2020. PMID: 33502003 Free PMC article.
-
Individual risk factors associated with SARS-CoV-2 infection during Alpha variant in high-income countries: a systematic review and meta-analysis.Front Public Health. 2024 Jul 30;12:1367480. doi: 10.3389/fpubh.2024.1367480. eCollection 2024. Front Public Health. 2024. PMID: 39139667 Free PMC article.
Cited by
-
Health Status and COVID-19 Epidemiology in an Inland Region of Portugal: A Retrospective Study.Int J Environ Res Public Health. 2024 Aug 6;21(8):1033. doi: 10.3390/ijerph21081033. Int J Environ Res Public Health. 2024. PMID: 39200643 Free PMC article.
-
Sociodemographic and Clinical Factors Associated with COVID-19 Mortality in India: a Retrospective Study.Acta Inform Med. 2025;33(1):23-29. doi: 10.5455/aim.2024.33.23-29. Acta Inform Med. 2025. PMID: 40223849 Free PMC article.
-
Application of MALDI-TOF MS and machine learning for the detection of SARS-CoV-2 and non-SARS-CoV-2 respiratory infections.Microbiol Spectr. 2024 May 2;12(5):e0406823. doi: 10.1128/spectrum.04068-23. Epub 2024 Mar 18. Microbiol Spectr. 2024. PMID: 38497716 Free PMC article.
References
-
- Ng OT, Marimuthu K, Koh V, Pang J, Linn KZ, Sun J, De Wang L, Chia WN, Tiu C, Chan M, Ling LM, Vasoo S, Abdad MY, Chia PY, Lee TH, Lin RJ, Sadarangani SP, Chen M-C, Said Z, Kurupatham L, Pung R, Wang L-F, Cook AR, Leo Y-S, Lee VJ. 2021. SARS-CoV-2 seroprevalence and transmission risk factors among high-risk close contacts: a retrospective cohort study. Lancet Infect Dis 21:333–343. doi:10.1016/S1473-3099(20)30833-1 - DOI - PMC - PubMed
-
- Levin AT, Owusu-Boaitey N, Pugh S, Fosdick BK, Zwi AB, Malani A, Soman S, Besançon L, Kashnitsky I, Ganesh S, McLaughlin A, Song G, Uhm R, Herrera-Esposito D, de Los Campos G, Peçanha Antonio ACP, Tadese EB, Meyerowitz-Katz G. 2022. Assessing the burden of COVID-19 in developing countries: systematic review, meta-analysis and public policy implications. BMJ Glob Health 7:e008477. doi:10.1136/bmjgh-2022-008477 - DOI - PMC - PubMed
-
- Corsi DJ, Subramanian SV, Chow CK, McKee M, Chifamba J, Dagenais G, Diaz R, Iqbal R, Kelishadi R, Kruger A, Lanas F, López-Jaramilo P, Mony P, Mohan V, Avezum A, Oguz A, Rahman MO, Rosengren A, Szuba A, Li W, Yusoff K, Yusufali A, Rangarajan S, Teo K, Yusuf S. 2013. Prospective urban rural epidemiology (PURE) study: baseline characteristics of the household sample and comparative analyses with national data in 17 countries. Am Heart J 166:636–646. doi:10.1016/j.ahj.2013.04.019 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
