

Isolating the Drivers of Racial Inequities in Prostate Cancer Treatment
- PMID: 38214587
- PMCID: PMC10922444
- DOI: 10.1158/1055-9965.EPI-23-0892
Isolating the Drivers of Racial Inequities in Prostate Cancer Treatment
Abstract
Background: Black individuals in the United States are less likely than White individuals to receive curative therapies despite a 2-fold higher risk of prostate cancer death. While research has described treatment inequities, few studies have investigated underlying causes.
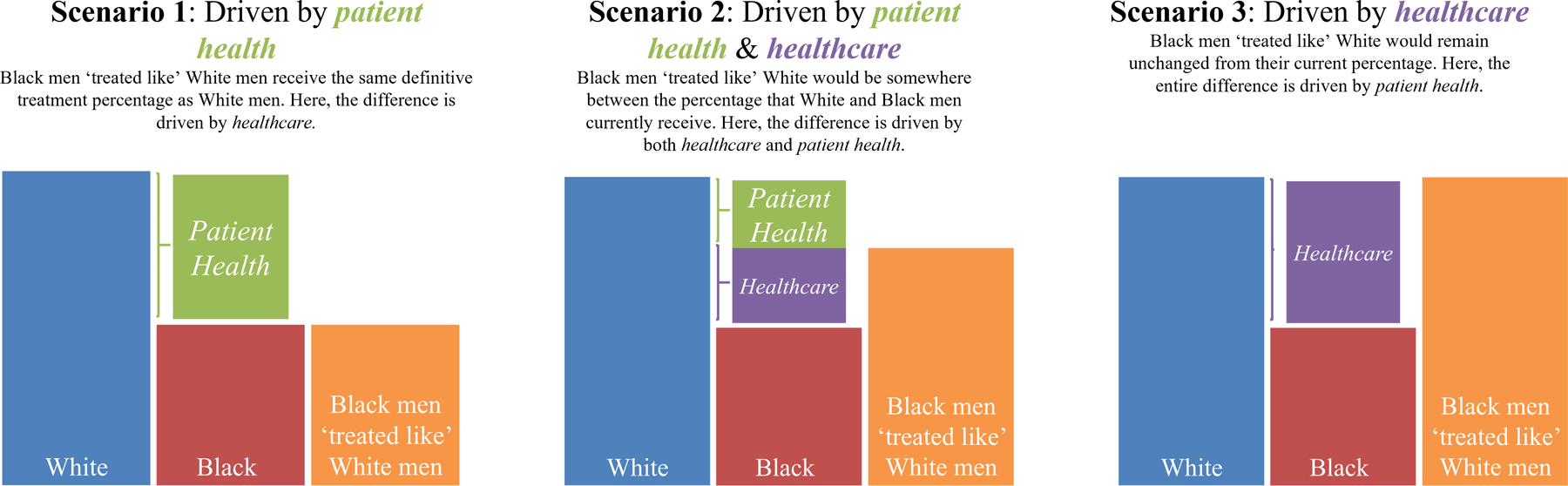
Methods: We analyzed a cohort of 40,137 Medicare beneficiaries (66 and older) linked to the Surveillance Epidemiology and End Results (SEER) cancer registry who had clinically significant, non-metastatic (cT1-4N0M0, grade group 2-5) prostate cancer (diagnosed 2010-2015). Using the Kitagawa-Oaxaca-Blinder decomposition, we assessed the contributions of patient health and health care delivery on the racial difference in localized prostate cancer treatments (radical prostatectomy or radiation). Patient health consisted of comorbid diagnoses, tumor characteristics, SEER site, diagnosis year, and age. Health care delivery was captured as a prediction model with these health variables as predictors of treatment, reflecting current treatment patterns.
Results: A total of 72.1% and 78.6% of Black and White patients received definitive treatment, respectively, a difference of 6.5 percentage points. An estimated 15% [95% confidence interval (CI): 6-24] of this treatment difference was explained by measured differences in patient health, leaving the remaining estimated 85% (95% CI: 74-94) attributable to a potentially broad range of health care delivery factors. Limitations included insufficient data to explore how specific health care delivery factors, including structural racism and social determinants, impact differential treatment.
Conclusions: Our results show the inadequacy of patient health differences as an explanation of the treatment inequity.
Impact: Investing in studies and interventions that support equitable health care delivery for Black individuals with prostate cancer will contribute to improved outcomes.
©2024 American Association for Cancer Research.
Conflict of interest statement
Conflicts of interest: The authors declare no potential conflicts of interest.
Figures


References
-
- . Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care (Smedley BD, Stith AY, Nelson AR, eds.). National Academies Press (US); 2003. Accessed June 9, 2023. http://www.ncbi.nlm.nih.gov/books/NBK220358/ - PubMed
-
- . National Academies of Sciences, Engineering, and Medicine, Health and Medicine Division, Board on Population Health and Public Health Practice, Committee on Community-Based Solutions to Promote Health Equity in the United States. Communities in Action: Pathways to Health Equity (Baciu A, Negussie Y, Geller A, Weinstein, eds.). National Academies Press (US); 2017. Accessed June 9, 2023. http://www.ncbi.nlm.nih.gov/books/NBK425848/ - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
