

Outcomes in people with eating disorders: a transdiagnostic and disorder-specific systematic review, meta-analysis and multivariable meta-regression analysis
- PMID: 38214616
- PMCID: PMC10785991
- DOI: 10.1002/wps.21182
Outcomes in people with eating disorders: a transdiagnostic and disorder-specific systematic review, meta-analysis and multivariable meta-regression analysis
Abstract
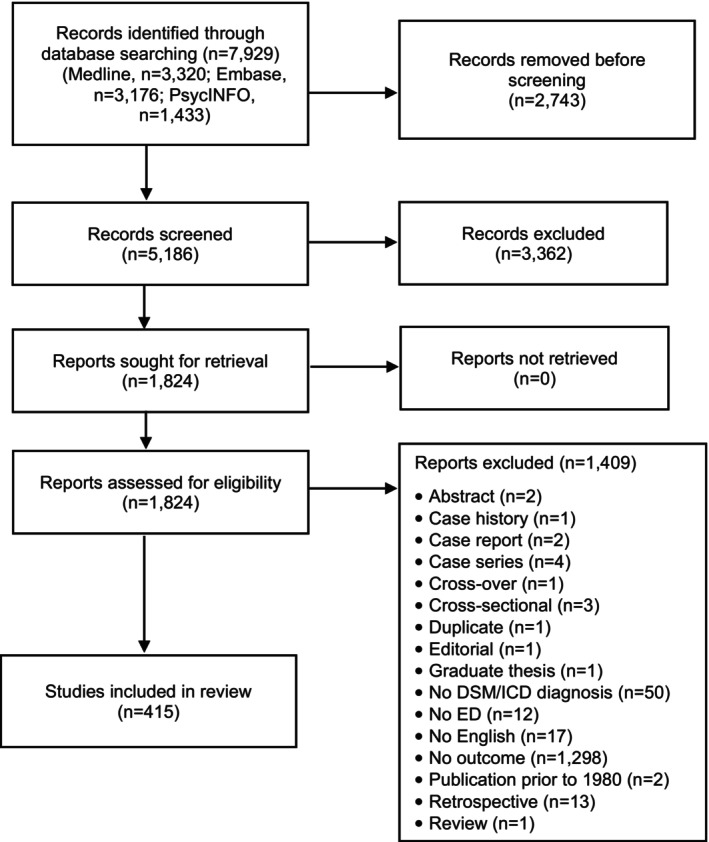
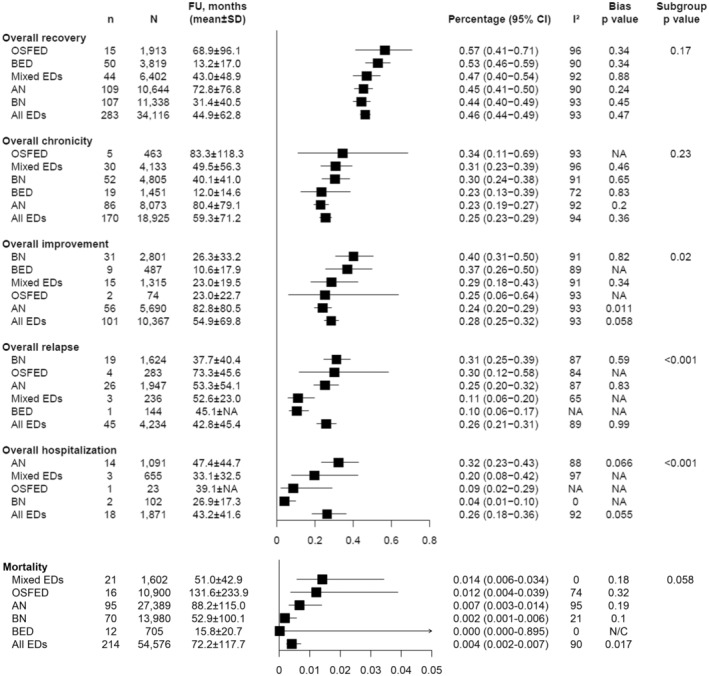
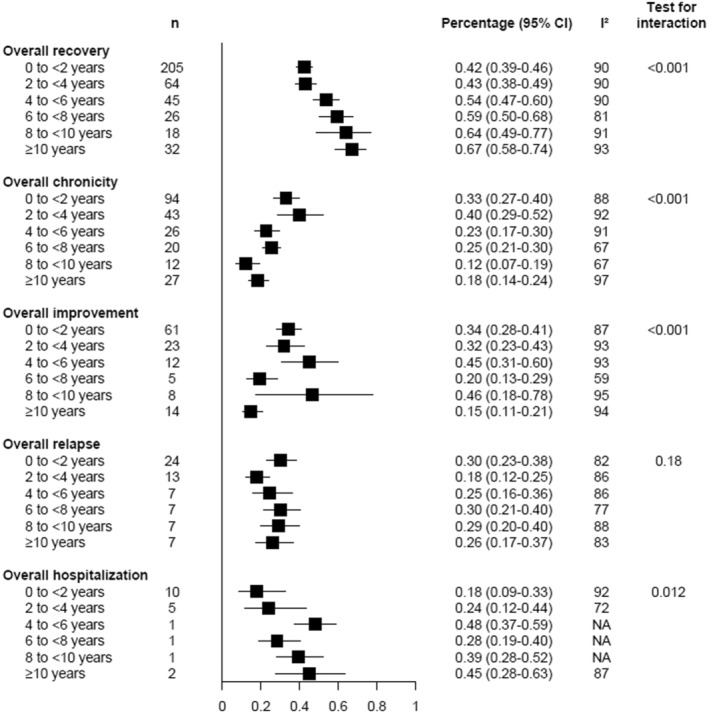
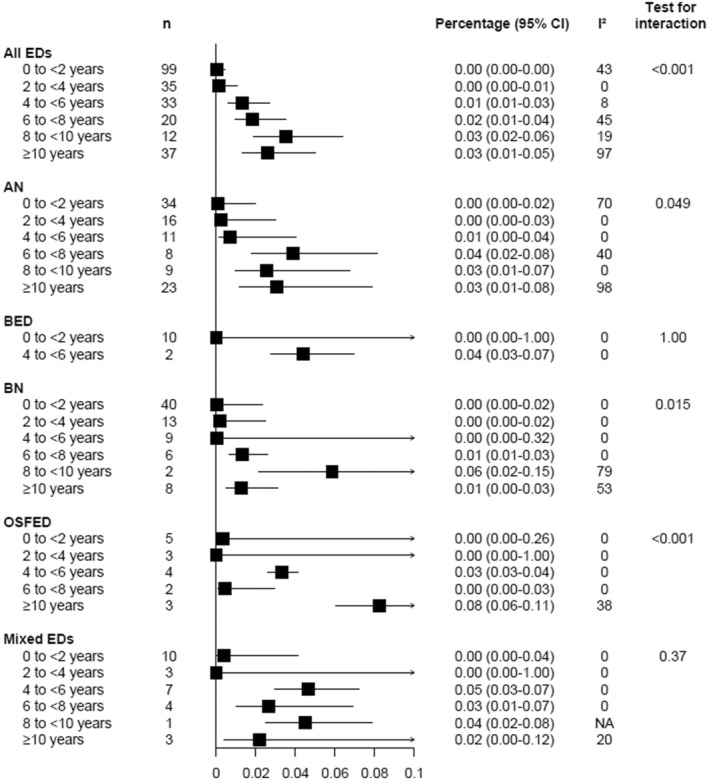
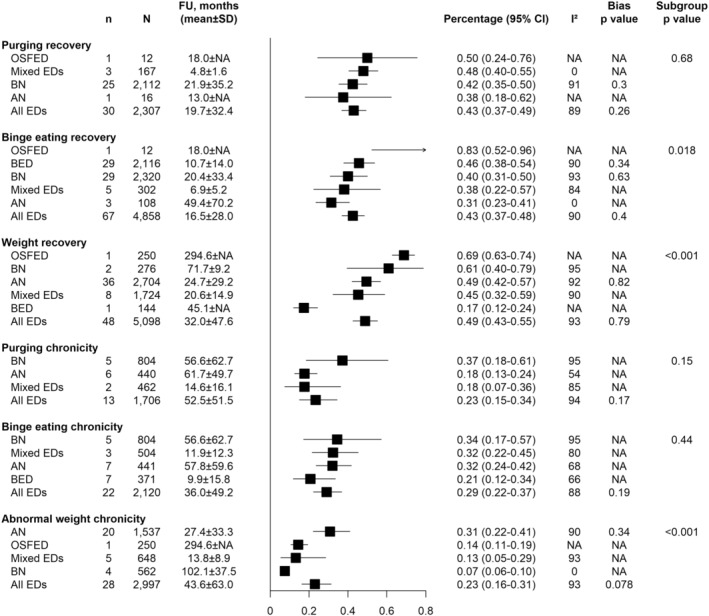
Eating disorders (EDs) are known to be associated with high mortality and often chronic and severe course, but a recent comprehensive systematic review of their outcomes is currently missing. In the present systematic review and meta-analysis, we examined cohort studies and clinical trials published between 1980 and 2021 that reported, for DSM/ICD-defined EDs, overall ED outcomes (i.e., recovery, improvement and relapse, all-cause and ED-related hospitalization, and chronicity); the same outcomes related to purging, binge eating and body weight status; as well as mortality. We included 415 studies (N=88,372, mean age: 25.7±6.9 years, females: 72.4%, mean follow-up: 38.3±76.5 months), conducted in persons with anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED), other specified feeding and eating disorders (OSFED), and/or mixed EDs, from all continents except Africa. In all EDs pooled together, overall recovery occurred in 46% of patients (95% CI: 44-49, n=283, mean follow-up: 44.9±62.8 months, no significant ED-group difference). The recovery rate was 42% at <2 years, 43% at 2 to <4 years, 54% at 4 to <6 years, 59% at 6 to <8 years, 64% at 8 to <10 years, and 67% at ≥10 years. Overall chronicity occurred in 25% of patients (95% CI: 23-29, n=170, mean follow-up: 59.3±71.2 months, no significant ED-group difference). The chronicity rate was 33% at <2 years, 40% at 2 to <4 years, 23% at 4 to <6 years, 25% at 6 to <8 years, 12% at 8 to <10 years, and 18% at ≥10 years. Mortality occurred in 0.4% of patients (95% CI: 0.2-0.7, n=214, mean follow-up: 72.2±117.7 months, no significant ED-group difference). Considering observational studies, the mortality rate was 5.2 deaths/1,000 person-years (95% CI: 4.4-6.1, n=167, mean follow-up: 88.7±120.5 months; significant difference among EDs: p<0.01, range: from 8.2 for mixed ED to 3.4 for BN). Hospitalization occurred in 26% of patients (95% CI: 18-36, n=18, mean follow-up: 43.2±41.6 months; significant difference among EDs: p<0.001, range: from 32% for AN to 4% for BN). Regarding diagnostic migration, 8% of patients with AN migrated to BN and 16% to OSFED; 2% of patients with BN migrated to AN, 5% to BED, and 19% to OSFED; 9% of patients with BED migrated to BN and 19% to OSFED; 7% of patients with OSFED migrated to AN and 10% to BN. Children/adolescents had more favorable outcomes across and within EDs than adults. Self-injurious behaviors were associated with lower recovery rates in pooled EDs. A higher socio-demographic index moderated lower recovery and higher chronicity in AN across countries. Specific treatments associated with higher recovery rates were family-based therapy, cognitive-behavioral therapy (CBT), psychodynamic therapy, and nutritional interventions for AN; self-help, CBT, dialectical behavioral therapy (DBT), psychodynamic therapy, nutritional and pharmacological treatments for BN; CBT, nutritional and pharmacological interventions, and DBT for BED; and CBT and psychodynamic therapy for OSFED. In AN, pharmacological treatment was associated with lower recovery, and waiting list with higher mortality. These results should inform future research, clinical practice and health service organization for persons with EDs.
Keywords: Eating disorders; anorexia nervosa; binge eating disorder; bulimia nervosa; chronicity; cognitive-behavioral therapy; diagnostic migration; family-based therapy; hospitalization; mortality; nutritional interventions; recovery.
© 2024 World Psychiatric Association.
Figures
References
-
- Mustelin L, Silén Y, Raevuori A et al. The DSM‐5 diagnostic criteria for anorexia nervosa may change its population prevalence and prognostic value. J Psychiatr Res 2016;77:85‐91. - PubMed
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders, 5th ed. Washington: American Psychiatric Association, 2013.
-
- World Health Organization . International classification of diseases, 11th ed. Geneva: World Health Organization, 2020.
LinkOut - more resources
Full Text Sources
