

Time Trends in Causes of Death in People With HIV: Insights From the Swiss HIV Cohort Study
- PMID: 38214897
- PMCID: PMC11259222
- DOI: 10.1093/cid/ciae014
Time Trends in Causes of Death in People With HIV: Insights From the Swiss HIV Cohort Study
Abstract
Background: Advancements in access to antiretroviral therapy (ART) and human immunodeficiency virus (HIV) care have led to a decline in AIDS-related deaths among people with HIV (PWH) in Switzerland. However, data on the ongoing changes in causes of death among PWH over the past 15 years are scarce.
Methods: We investigated all reported deaths in the Swiss HIV Cohort Study between 2005 and 2022. Causes of death were categorized using the Coding Causes of Death in HIV protocol. The statistical analysis included demographic stratification to identify time trends and logistic regression models to determine associated factors for the underlying cause of death.
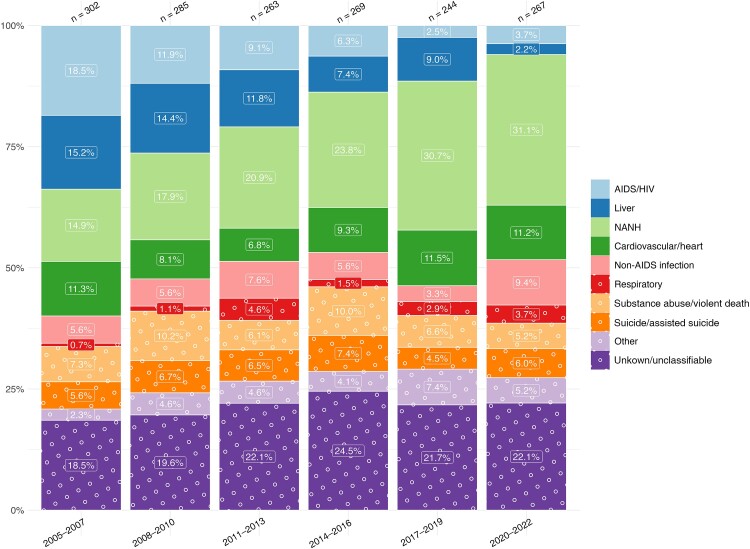
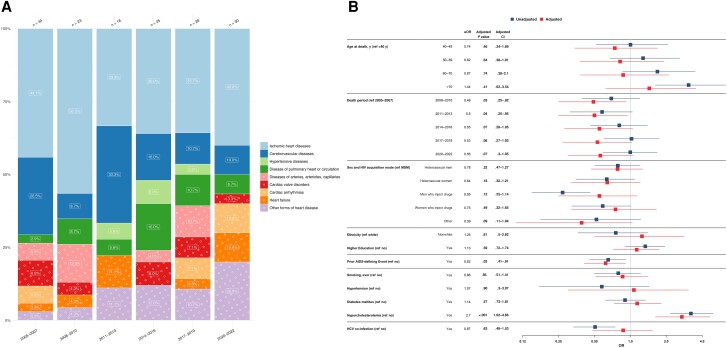
Results: In total, 1630 deaths were reported, with 23.7% of individuals assigned female sex at birth. These deaths included 147 (9.0%) HIV/AIDS-related deaths, 373 (22.9%) due to non-AIDS, non-hepatic cancers, 166 (10.2%) liver-related deaths, and 158 (9.7%) cardiovascular-related deaths. The median age at death (interquartile range) increased from 45.0 (40.0-53.0) years in 2005-2007 to 61.0 (56.0-69.5) years in 2020-2022. HIV/AIDS- and liver-related deaths decreased, whereas deaths from non-AIDS, non-hepatic cancers increased and cardiovascular-related deaths remained relatively stable.
Conclusions: The proportionally decreasing HIV/AIDS and liver-related deaths showcase the effectiveness of ART, comprehensive HIV patient care, and interventions targeting hepatitis C virus coinfection. Future research should focus on managing cancer and cardiovascular-related conditions as the new leading causes of death among PWH. Comprehensive healthcare strategies focusing on non-AIDS-related comorbid conditions, cancer management, and sustaining liver and cardiovascular health are needed to bridge the ongoing health disparities between PWH and the general population.
Keywords: HIV/AIDS; cancer; cardiovascular risk; cause of death; hepatitis.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest . M. S. R. W. has received conference travel grants from Gilead. J. J. D. R. has received educational research grants to their institution from Gilead Sciences and ViiV healthcare, unrelated to the present work. M. H. received travel grants from Gilead Science, ViiV Healthcare and MSD; lecture honoraria for conference report from Gilead Science and ViiV Healthcare; and payment for expert testimony from ViiV Healthcare and Gilead Science, all unrelated to the present work. M. C.'s institution received research grants from Gilead, MSD and ViiV healthcare; reports payment for expert testimony from MSD, Gilead, and ViiV; and travel grants from Gilead. E. B's institution received a research grant from MSD, fees for E. B.'s participation on advisory boards and/or travel grants from Gilead, ViiV, MSD, AbbVie, Pfizer, AstraZeneca, Moderna, and Ely Lilly; E. B. also reports consulting fees from Moderna and payment or honoraria from Pfizer. E. H. received financial support for attending meetings from Gilead Sciences, ViiV healthcare, and AstraZeneca; the travel grants were paid to her institution. H. F. received educational grants from ViiV, MSD, AbbVie, Gilead, Sandoz, AstraZeneca and Pfizer, paid to his institution. M. S. received money for advisory boards and/or travel grants from Gilead, ViiV, and MSD, paid to his institution, and reports an unpaid leadership or fiduciary role with the SHCS. P. S.'s institution has received travel grants, congress, and advisory fees from ViiV and Gilead, unrelated to the present work. D. H. has received consultancies from AstraZeneca, Gilead, ViiV Healthcare, and Bavarian Nordic, as well as institutional funding from AbbVie, AstraZeneca, Gilead, GSK, MSD, Pfizer, Roche, ViiV Healthcare; reports support for travel and/or attending meetings from Gilead; and reports leadership or fidicuary roles with Patient Focused Medicines Development (PFMD) and Positive Council Switzerland. D. L. B. reports honoraria for advisory boards or speaker lectures, paid to himself, from Gilead, MSD, Pfizer, and ViiV and support for attending meetings and/or travel from Gilead and ViiV, unrelated to the present work. H. F. G. has received honoraria for data and safety monitoring board or advisory board membership from Merck, Gilead Sciences, ViiV Healthcare, GSK, Janssen, Johnson & Johnson, and Novartis and a travel grant from Gilead Sciences. He also reports unrestricted research grants from Gilead Sciences; grants or contracts paid to his institution from the Swiss National Science Foundation, the SCHS, and the National Institutes of Health; and unrestricted research grants from Gilead sciences and the Yvonne Jacob Foundation. All other authors report no potential conflicts All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Weber R, Ruppik M, Rickenbach M, et al. Decreasing mortality and changing patterns of causes of death in the Swiss HIV Cohort Study. HIV Med 2013; 14:195–207. - PubMed
-
- Trickey A, McGinnis K, John Gill M, et al. Causes of death among adults with HIV on ART in Europe and North America: 1996–2019. 2023. Available at: https://www.croiconference.org/abstract/causes-of-death-among-adults-wit.... Accessed 31 August 2023.
-
- Lohse N, Hansen AB, Pedersen G, et al. Survival of persons with and without HIV infection in Denmark, 1995–2005. Ann Intern Med 2007; 146:87–95. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
