

Novel rapid method for identifying and quantifying pathogenic bacteria within four hours of blood collection
- PMID: 38216600
- PMCID: PMC10786899
- DOI: 10.1038/s41598-023-50864-0
Novel rapid method for identifying and quantifying pathogenic bacteria within four hours of blood collection
Abstract
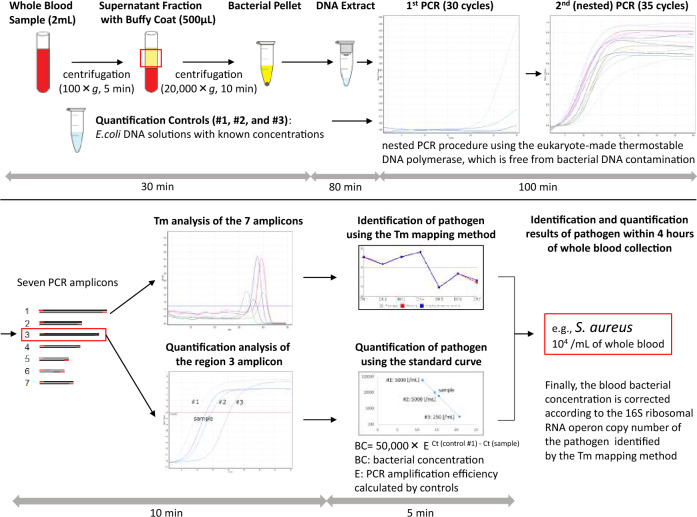
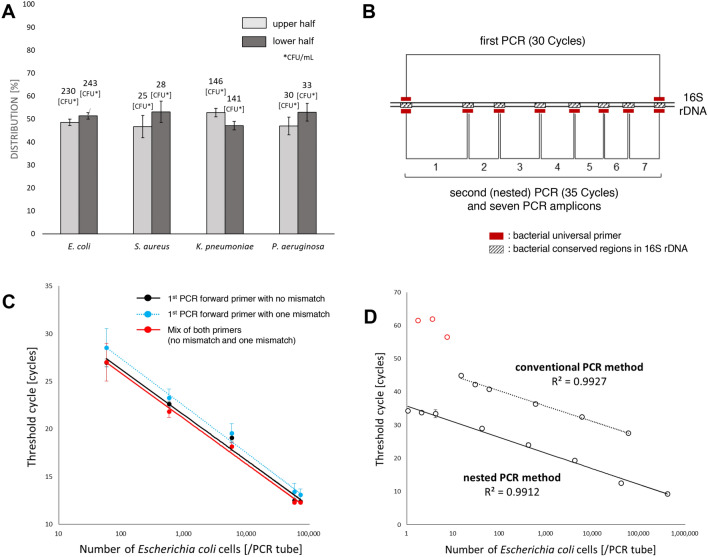
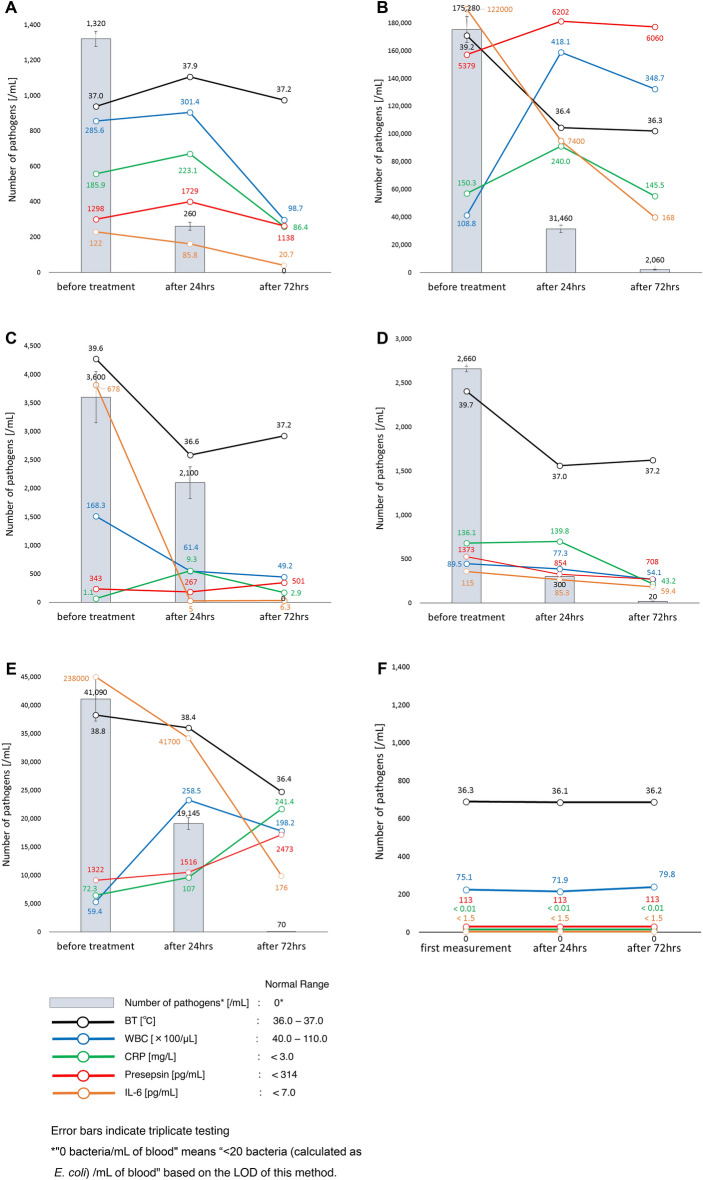
Sepsis is life-threatening organ dysfunction and is considered a major cause of health loss. However, since the current biomarkers of sepsis reflect the host's immune response to microorganisms, they would inevitably cause a time-lag. This means that there is still no truly reliable biomarker of sepsis. In the present study, we developed a novel method for identifying and quantifying unknown pathogenic bacteria within four hours of sample collection. The most important point of this study is that the novel method can be used to determine the number of bacteria in a sample as a novel biomarker of infectious diseases. Indeed, based on the number of bacteria, we were able to accurately estimate the severity of microbial infection. Furthermore, using the time-dependent changes in the number of bacteria, we were able to monitor the therapeutic effect accurately. The rapid identification and quantification of bacteria may change our approach to medical care.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
