Diagnostic accuracy of research criteria for prodromal frontotemporal dementia
- PMID: 38216961
- PMCID: PMC10785469
- DOI: 10.1186/s13195-024-01383-1
Diagnostic accuracy of research criteria for prodromal frontotemporal dementia
Abstract
Background: The Genetic Frontotemporal Initiative Staging Group has proposed clinical criteria for the diagnosis of prodromal frontotemporal dementia (FTD), termed mild cognitive and/or behavioral and/or motor impairment (MCBMI). The objective of the study was to validate the proposed research criteria for MCBMI-FTD in a cohort of genetically confirmed FTD cases against healthy controls.
Methods: A total of 398 participants were enrolled, 117 of whom were carriers of an FTD pathogenic variant with mild clinical symptoms, while 281 were non-carrier family members (healthy controls (HC)). A subgroup of patients underwent blood neurofilament light (NfL) levels and anterior cingulate atrophy assessment.
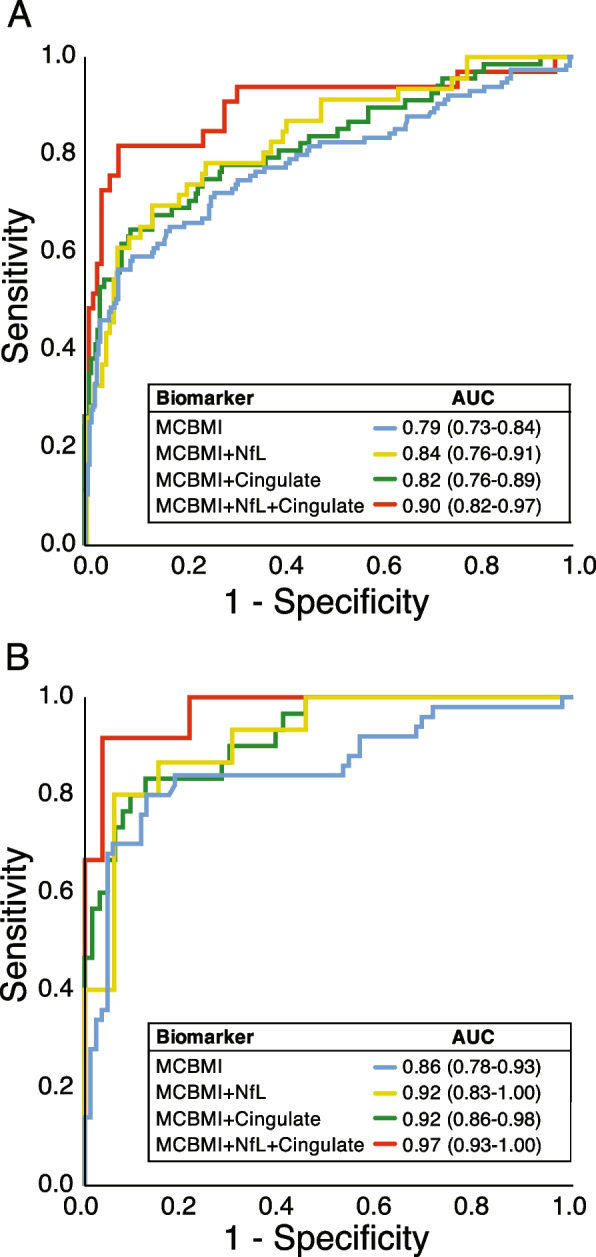
Results: The core clinical criteria correctly classified MCBMI vs HC with an AUC of 0.79 (p < 0.001), while the addition of either blood NfL or anterior cingulate atrophy significantly increased the AUC to 0.84 and 0.82, respectively (p < 0.001). The addition of both markers further increased the AUC to 0.90 (p < 0.001).
Conclusions: The proposed MCBMI criteria showed very good classification accuracy for identifying the prodromal stage of FTD.
Keywords: Diagnostic accuracy; Diagnostic criteria; Frontotemporal dementia; MCBMI; Prodromal.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures