

Understanding mechanisms of racial disparities in breast cancer: an assessment of screening and regular care in the Carolina Breast Cancer Study
- PMID: 38217760
- PMCID: PMC11045315
- DOI: 10.1007/s10552-023-01833-5
Understanding mechanisms of racial disparities in breast cancer: an assessment of screening and regular care in the Carolina Breast Cancer Study
Abstract
Purpose: Screening history influences stage at detection, but regular preventive care may also influence breast tumor diagnostic characteristics. Few studies have evaluated healthcare utilization (both screening and primary care) in racially diverse screening-eligible populations.
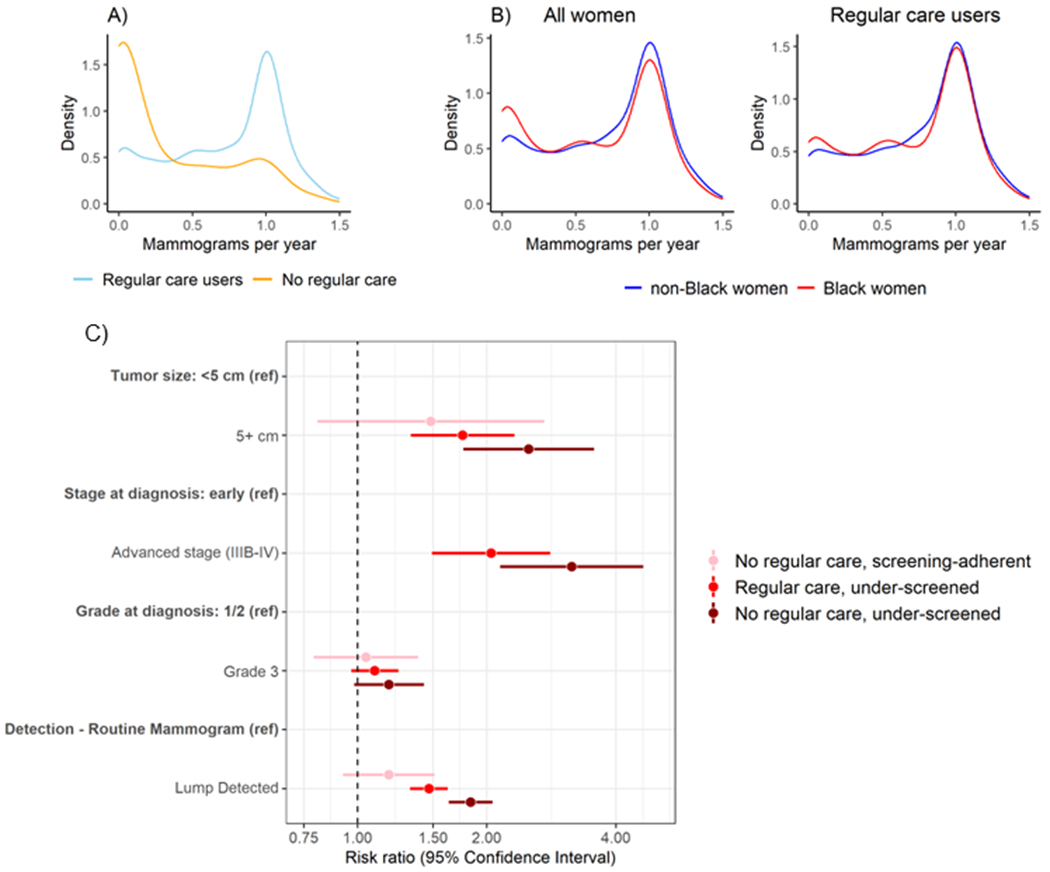
Methods: This analysis included 2,058 women age 45-74 (49% Black) from the Carolina Breast Cancer Study, a population-based cohort of women diagnosed with invasive breast cancer between 2008 and 2013. Screening history (threshold 0.5 mammograms per year) and pre-diagnostic healthcare utilization (i.e. regular care, based on responses to "During the past ten years, who did you usually see when you were sick or needed advice about your health?") were assessed as binary exposures. The relationship between healthcare utilization and tumor characteristics were evaluated overall and race-stratified.
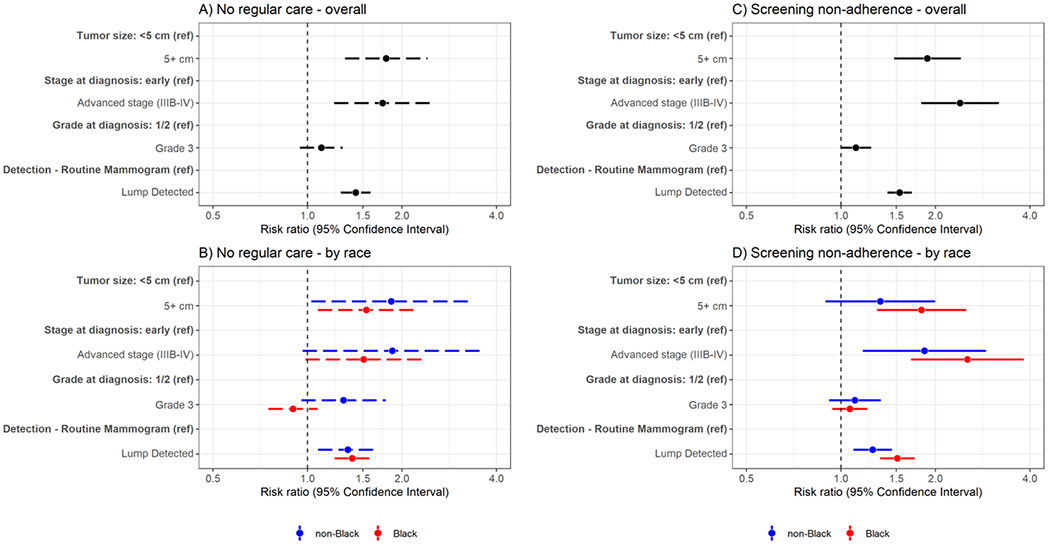
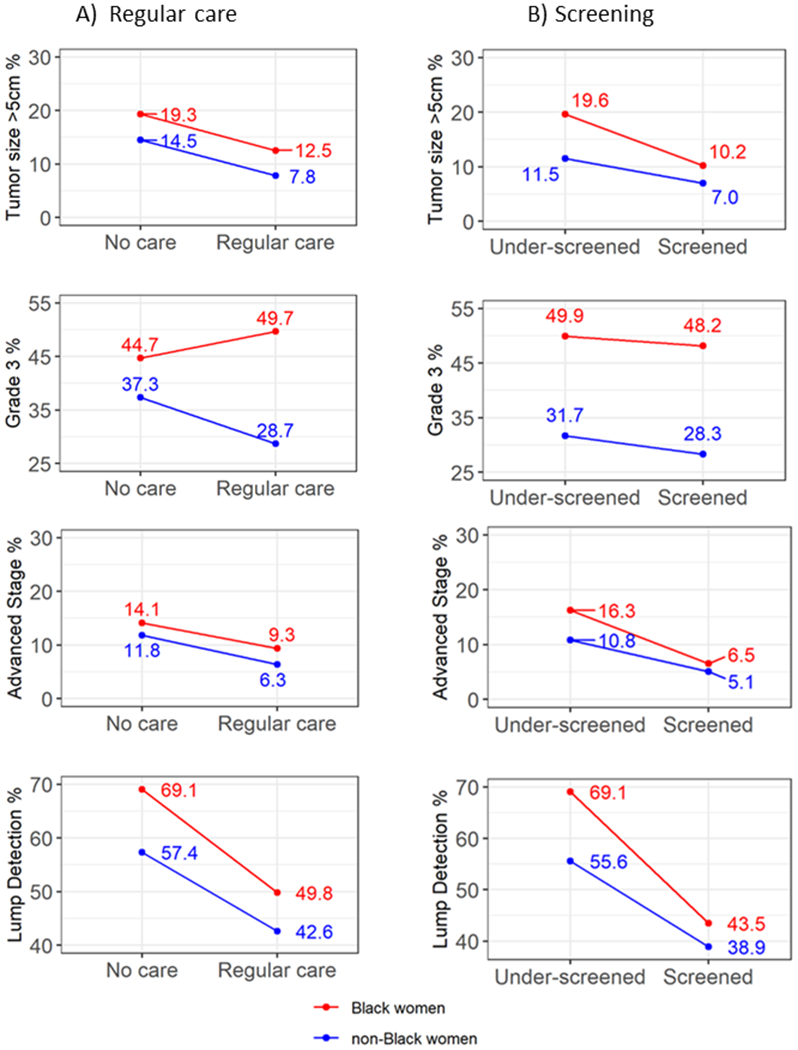
Results: Among those lacking screening, Black participants had larger tumors (5 + cm) (frequency 19.6% vs 11.5%, relative frequency difference (RFD) = 8.1%, 95% CI 2.8-13.5), but race differences were attenuated among screening-adherent participants (10.2% vs 7.0%, RFD = 3.2%, 0.2-6.2). Similar trends were observed for tumor stage and mode of detection (mammogram vs lump). Among all participants, those lacking both screening and regular care had larger tumors (21% vs 8%, RR = 2.51, 1.76-3.56) and advanced (3B +) stage (19% vs 6%, RR = 3.15, 2.15-4.63) compared to the referent category (screening-adherent and regular care). Under-use of regular care and screening was more prevalent in socioeconomically disadvantaged areas of North Carolina.
Conclusions: Access to regular care is an important safeguard for earlier detection. Our data suggest that health equity interventions should prioritize both primary care and screening.
Keywords: Cancer screening; Cohort study; Disparities; Healthcare; Mammography; Tumor presentation.
© 2024. The Author(s), under exclusive licence to Springer Nature Switzerland AG.
Conflict of interest statement
Figures
Similar articles
-
A latent class assessment of healthcare access factors and disparities in breast cancer care timeliness.PLoS Med. 2024 Dec 2;21(12):e1004500. doi: 10.1371/journal.pmed.1004500. eCollection 2024 Dec. PLoS Med. 2024. PMID: 39621782 Free PMC article.
-
Screening for breast cancer: a systematic review update to inform the Canadian Task Force on Preventive Health Care guideline.Syst Rev. 2024 Dec 19;13(1):304. doi: 10.1186/s13643-024-02700-3. Syst Rev. 2024. PMID: 39702409 Free PMC article.
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
Prophylactic mastectomy for the prevention of breast cancer.Cochrane Database Syst Rev. 2004 Oct 18;(4):CD002748. doi: 10.1002/14651858.CD002748.pub2. Cochrane Database Syst Rev. 2004. Update in: Cochrane Database Syst Rev. 2010 Nov 10;(11):CD002748. doi: 10.1002/14651858.CD002748.pub3. PMID: 15495033 Updated.
-
Racial and ethnic disparities in fecundability: a North American preconception cohort study.Hum Reprod. 2025 Jun 1;40(6):1183-1194. doi: 10.1093/humrep/deaf067. Hum Reprod. 2025. PMID: 40246287
Cited by
-
A latent class assessment of healthcare access factors and disparities in breast cancer care timeliness.PLoS Med. 2024 Dec 2;21(12):e1004500. doi: 10.1371/journal.pmed.1004500. eCollection 2024 Dec. PLoS Med. 2024. PMID: 39621782 Free PMC article.
-
Associations between social drivers of health and breast cancer stage at diagnosis among U.S. Black women.NPJ Breast Cancer. 2025 Aug 6;11(1):85. doi: 10.1038/s41523-025-00804-0. NPJ Breast Cancer. 2025. PMID: 40770199 Free PMC article.
-
Genomic Analysis Reveals Racial and Age-Related Differences in the Somatic Landscape of Breast Cancer and the Association with Socioeconomic Factors.Cancer Res. 2025 Apr 3;85(7):1327-1340. doi: 10.1158/0008-5472.CAN-24-1788. Cancer Res. 2025. PMID: 39879109
-
Applying a Novel Measure of Community-Level Healthcare Access to Assess Breast Cancer Care Timeliness.Cancer Epidemiol Biomarkers Prev. 2025 Jul 1;34(7):1199-1209. doi: 10.1158/1055-9965.EPI-25-0011. Cancer Epidemiol Biomarkers Prev. 2025. PMID: 40298936
References
-
- US Preventive Services Task Force. Draft Recommendation: Breast Cancer: Screening | United States Preventive Services Taskforce. Published May 9, 2023. Accessed May 28, 2023. https://www.uspreventiveservicestaskforce.org/uspstf/draft-recommendatio...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
