

Outcomes after surgical revascularization in diabetic patients
- PMID: 38218725
- PMCID: PMC10850843
- DOI: 10.1093/icvts/ivae014
Outcomes after surgical revascularization in diabetic patients
Abstract
Objectives: Patients with diabetes mellitus (DM) undergoing coronary artery bypass grafting (CABG) have been repeatedly demonstrated to have worse clinical outcomes compared to patients without DM. The objective of this study was to evaluate the impact of DM on 1-year clinical outcomes after isolated CABG.
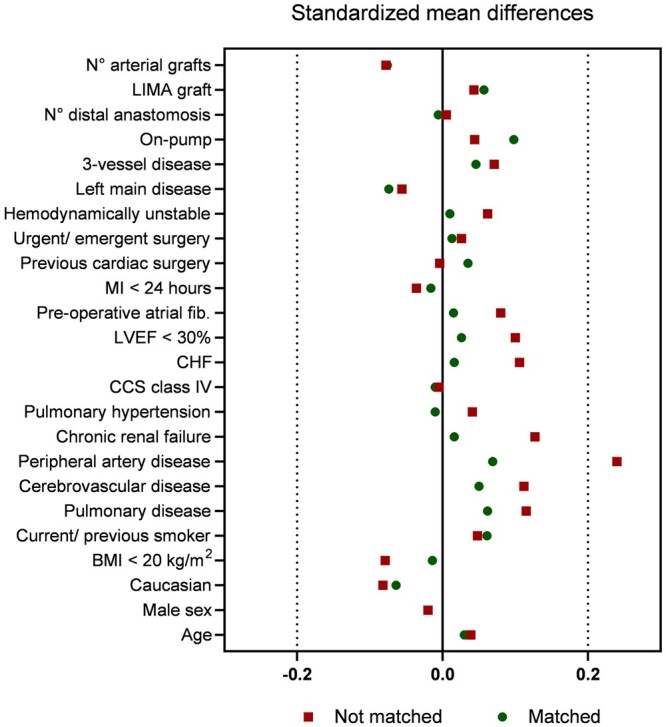
Methods: The European DuraGraft registry included 1130 patients (44.6%) with and 1402 (55.4%) patients without DM undergoing isolated CABG. Intra-operatively, all free venous and arterial grafts were treated with an endothelial damage inhibitor. Primary end point in this analysis was the incidence of a major adverse cardiac event (MACE), a composite of all-cause death, repeat revascularization or myocardial infarction at 1 year post-CABG. To balance between differences in baseline characteristics (n = 1072 patients in each group), propensity score matching was used. Multivariable Cox proportional hazards regression was performed to identify independent predictors of MACE.
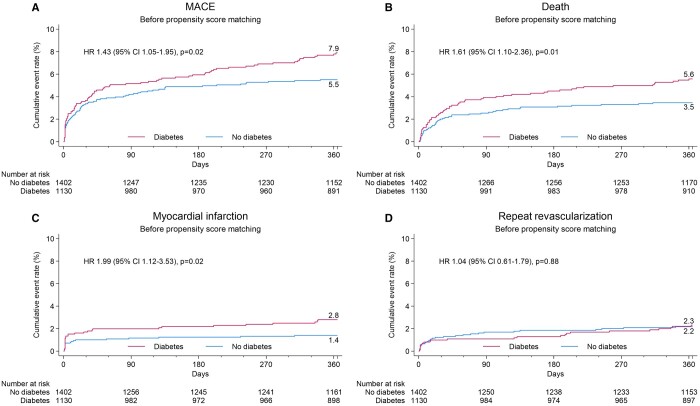
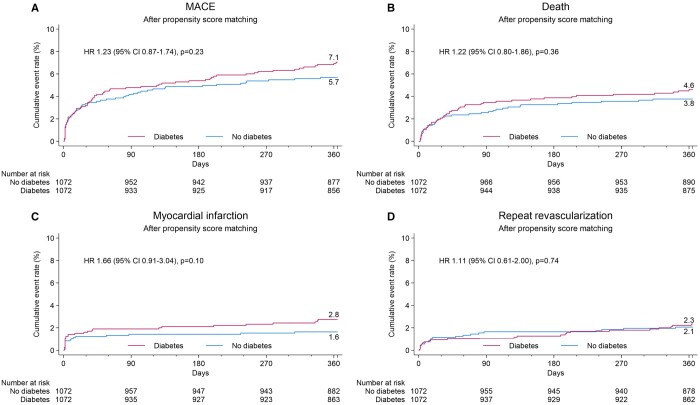
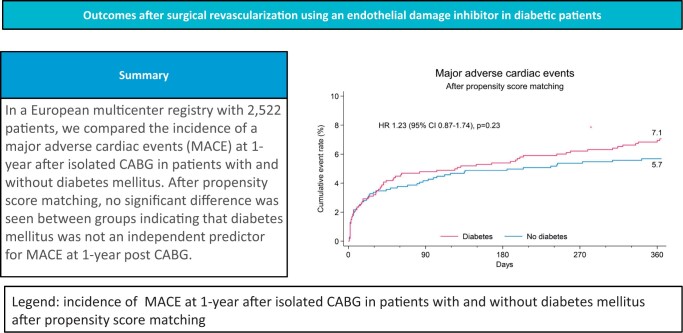
Results: Diabetic patients had a higher cardiovascular risk profile and EuroSCORE II with overall more comorbidities. Patients were comparable in regard to surgical techniques and completeness of revascularization. At 1 year, diabetics had a higher MACE rate {7.9% vs 5.5%, hazard ratio (HR) 1.43 [95% confidence interval (CI) 1.05-1.95], P = 0.02}, driven by increased rates of death [5.6% vs 3.5%, HR 1.61 (95% CI 1.10-2.36), P = 0.01] and myocardial infarction [2.8% vs 1.4%, HR 1.99 (95% CI 1.12-3.53) P = 0.02]. Following propensity matching, no statistically significant difference was found for MACE [7.1% vs 5.7%, HR 1.23 (95% CI 0.87-1.74) P = 0.23] or its components. Age, critical operative state, extracardiac arteriopathy, ejection fraction ≤50% and left main disease but not DM were identified as independent predictors for MACE.
Conclusions: In this study, 1-year outcomes in diabetics undergoing isolated CABG were comparable to patients without DM.
Keywords: Coronary artery bypass grafting; Diabetes mellitus; Endothelial damage inhibitor; Graft failure.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
References
-
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM. et al.; GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group. Global burden of cardiovascular diseases and risk factors, 1990–2019 update from the GBD 2019 study. J Am Coll Cardiol 2020;76:2982–3021. - PMC - PubMed
-
- Lüscher TF, Creager MA, Beckman JA, Cosentino F.. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part II. Circulation 2003;108:1655–61. - PubMed
-
- Sousa-Uva M, Neumann F-J, Ahlsson A, Alfonso F, Banning AP, Benedetto U. et al.; ESC Scientific Document Group. 2018 ESC/EACTS Guidelines on myocardial revscularization. The Task Force on myocardial revascularization of the European Society of Cardiology (ESC) and European Association for Cardio-Thoracic Surgery (EACTS). Eur J Cardiothorac Surg 2019;55:4–90. - PubMed
-
- Zhao DX, Leacche M, Balaguer JM, Boudoulas KD, Damp JA, Greelish JP. et al.; Writing Group of the Cardiac Surgery, Cardiac Anesthesiology, and Interventional Cardiology Groups at the Vanderbilt Heart and Vascular Institute. Routine intraoperative completion angiography after coronary artery bypass grafting and 1-stop hybrid revascularization results from a fully integrated hybrid catheterization laboratory/operating room. J Am Coll Cardiol 2009;53:232–41. - PubMed
-
- Caliskan E, de Souza DR, Böning A. et al. Saphenous vein grafts in contemporary coronary artery bypass graft surgery. Nat Rev Cardiol. 2020. Mar;17(3):155–169. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
