

AI improves accuracy, agreement and efficiency of pathologists for Ki67 assessments in breast cancer
- PMID: 38218973
- PMCID: PMC10787826
- DOI: 10.1038/s41598-024-51723-2
AI improves accuracy, agreement and efficiency of pathologists for Ki67 assessments in breast cancer
Abstract
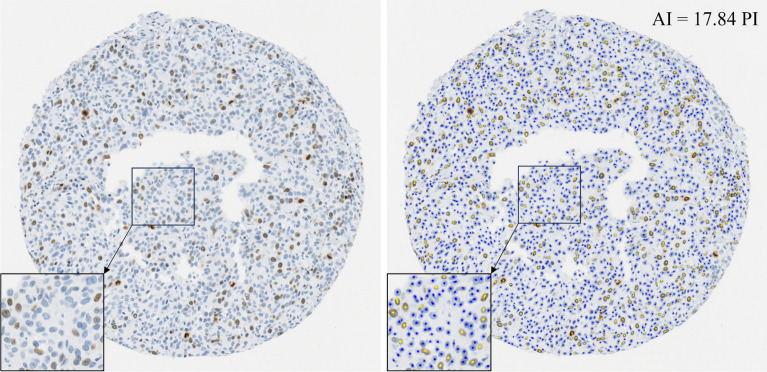
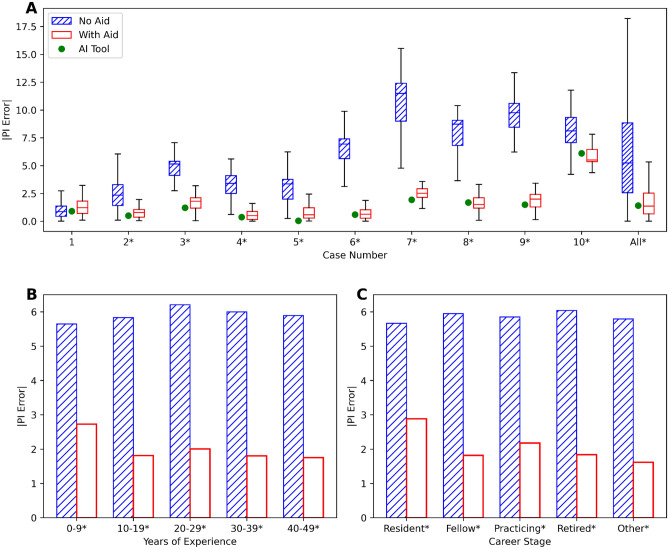
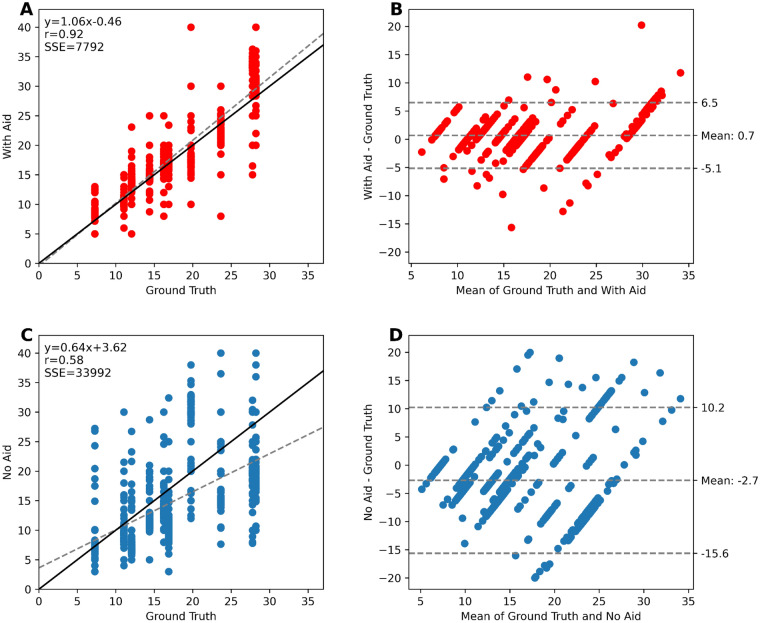
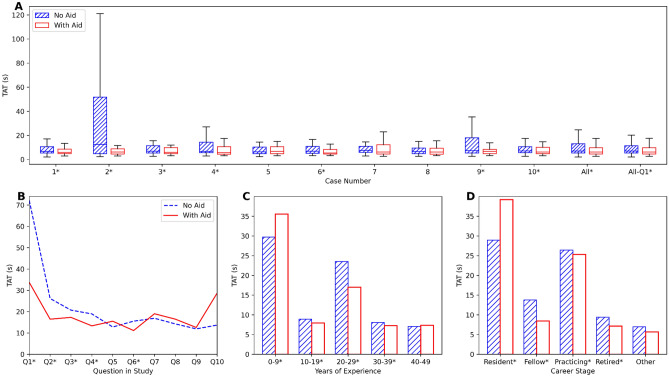
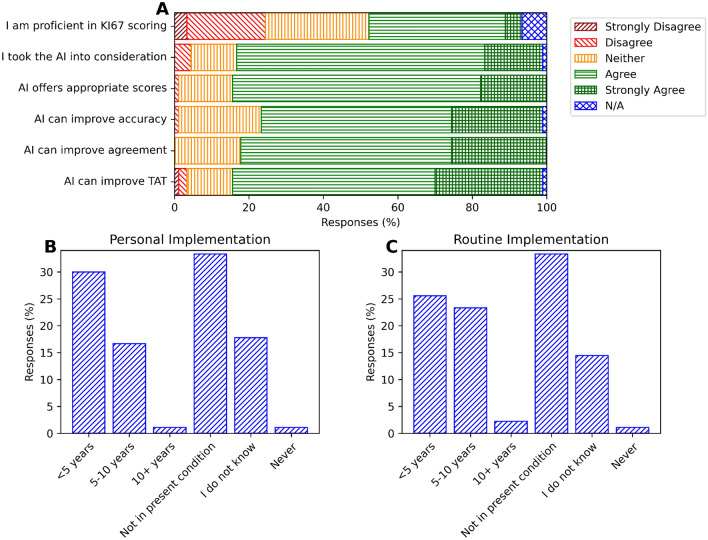
The Ki-67 proliferation index (PI) guides treatment decisions in breast cancer but suffers from poor inter-rater reproducibility. Although AI tools have been designed for Ki-67 assessment, their impact on pathologists' work remains understudied. 90 international pathologists were recruited to assess the Ki-67 PI of ten breast cancer tissue microarrays with and without AI. Accuracy, agreement, and turnaround time with and without AI were compared. Pathologists' perspectives on AI were collected. Using AI led to a significant decrease in PI error (2.1% with AI vs. 5.9% without AI, p < 0.001), better inter-rater agreement (ICC: 0.70 vs. 0.92; Krippendorff's α: 0.63 vs. 0.89; Fleiss' Kappa: 0.40 vs. 0.86), and an 11.9% overall median reduction in turnaround time. Most pathologists (84%) found the AI reliable. For Ki-67 assessments, 76% of respondents believed AI enhances accuracy, 82% said it improves consistency, and 83% trust it will improve efficiency. This study highlights AI's potential to standardize Ki-67 scoring, especially between 5 and 30% PI-a range with low PI agreement. This could pave the way for a universally accepted PI score to guide treatment decisions, emphasizing the promising role of AI integration into pathologist workflows.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Johnston SRD, et al. Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): Results from a preplanned interim analysis of a randomised, open-label, phase 3 trial. Lancet Oncol. 2023;24:77–90. doi: 10.1016/S1470-2045(22)00694-5. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
