

Efficacy of Calcium Enriched Mixture Cement, Mineral Trioxide Aggregate and Calcium Hydroxide Used as Direct Pulp Capping Agents in Deep Carious Lesions - A Randomised Clinical Trial
- PMID: 38219032
- PMCID: PMC10500208
- DOI: 10.14744/eej.2023.83007
Efficacy of Calcium Enriched Mixture Cement, Mineral Trioxide Aggregate and Calcium Hydroxide Used as Direct Pulp Capping Agents in Deep Carious Lesions - A Randomised Clinical Trial
Abstract
Objective: The primary objective of this randomised clinical trial was to evaluate the efficacy of Calcium Enriched Mixture (CEM) cement compared to Mineral Trioxide Aggregate (MTA) and Calcium Hydroxide (CH) in maintaining pulp vitality when used for direct pulp capping (DPC) of deep carious lesions with reversible pulpitis and secondary objective was to assess the overall success of DPC in carious exposures.
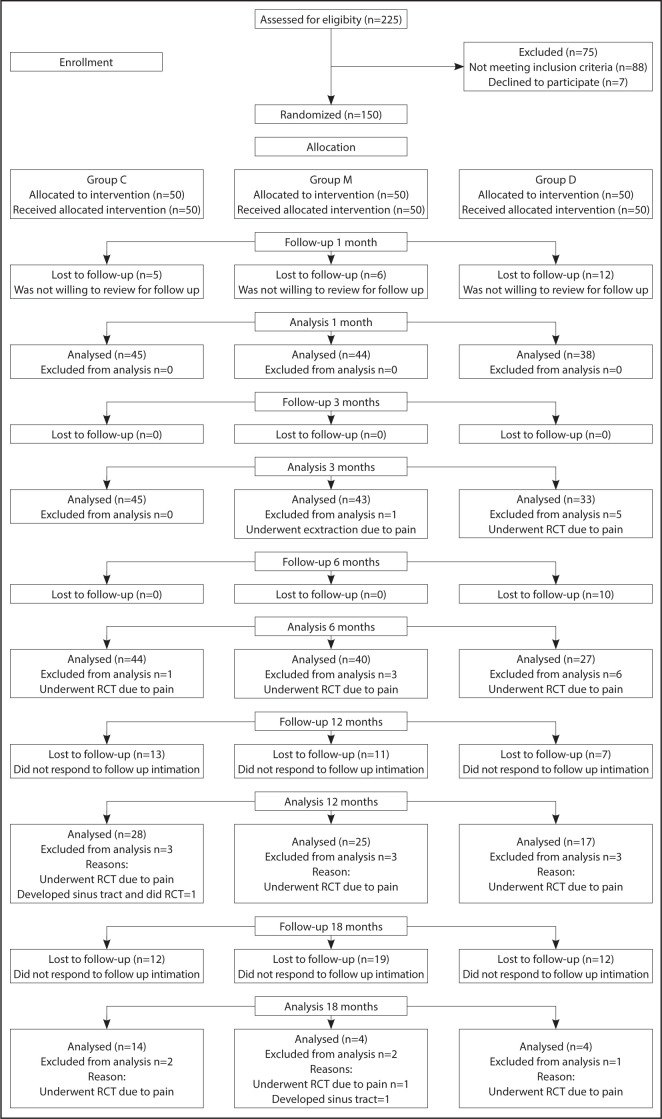
Methods: One hundred and fifty patients diagnosed with reversible pulpitis with deep carious lesions were included in this study. Patients were randomly allocated into three groups (n=50), Group C: CEM group, Group M: MTA group, and Group D: CH (Dycal) group. After caries removal by mechanical excavation except for one carious spot, the removal of which resulted in the exposure of the pulp, the final carious spot was removed with a sterile no.2 round carbide bur. After haemostasis, the pulpal wound was dressed by a capping agent, followed immediately by permanent restoration. Patients were assessed for successful outcomes based on positive vitality tests, absence of clinical signs and symptoms, and PAI scores after 1, 3, 6, 12, and 18-month follow-up periods. The ANOVA test was employed to analyse quantitative variables, and the Pearson Chi-square test was used for qualitative variables. A Bonferroni Test was employed as the post hoc test for intergroup comparison. The significance level was set at p≤0.05 within all tests.
Results: The percentage of success in Group C was 86.7%, Group M was 77.3%, and Group D was 57.9%. This study's overall success rate after direct pulp capping of deep carious lesions was 74.8%. A statistically significant difference in PAI score was found between Groups C and D. Pain on percussion and response to vitality tests also showed significant differences among the three groups at the one-month follow-up.
Conclusion: CEM cement had comparable efficacy to MTA and was superior to CH in maintaining pulpal vitality following DPC in teeth with reversible pulpitis. An overall success rate of 74.8% indicated that DPC in deep carious lesions with reversible pulpitis could yield favourable clinical outcomes. (EEJ-2022-11-134).
Conflict of interest statement
The authors deny any conflict of interest.
Figures











References
-
- Wolters WJ, Duncan HF, Tomson PL, Karim IE, McKenna G, Dorri M, et al. Minimally invasive endodontics: a new diagnostic system for assessing pulpitis and subsequent treatment needs. Int Endod J. 2017;50(9):825–9. - PubMed
-
- American Academy on Pediatric Dentistry Clinical Affairs Committee-Pulp Therapy subcommittee, American Academy on Pediatric Dentistry Council on Clinical Affairs Guideline on pulp therapy for primary and young permanent teeth. Pediatr Dent. 2008-2009;30(Suppl 7):170–4. - PubMed
-
- Camps J, Fuks AB. Pediatric endodontics: endodontic treatment for the primary and young permanent dentition. In: Cohen S, Hargreaves K, Keiser K, editors. Pathways of the pulp. 9th ed. St Luois: Mosby Elsevier; 2006. pp. 822–82.
-
- Tronstad L, Mjör IA. Capping of the inflamed pulp. Oral Surg Oral Med Oral Pathol. 1972;34(3):477–85. - PubMed
-
- Langeland K. Management of the inflamed pulp associated with deep carious lesion. J Endod. 1981;7(4):169–81. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
