

Usefulness of Robotic Stereotactic Assistance (ROSA®) Device for Stereoelectroencephalography Electrode Implantation: A Systematic Review and Meta-analysis
- PMID: 38220166
- PMCID: PMC10918457
- DOI: 10.2176/jns-nmc.2023-0119
Usefulness of Robotic Stereotactic Assistance (ROSA®) Device for Stereoelectroencephalography Electrode Implantation: A Systematic Review and Meta-analysis
Abstract
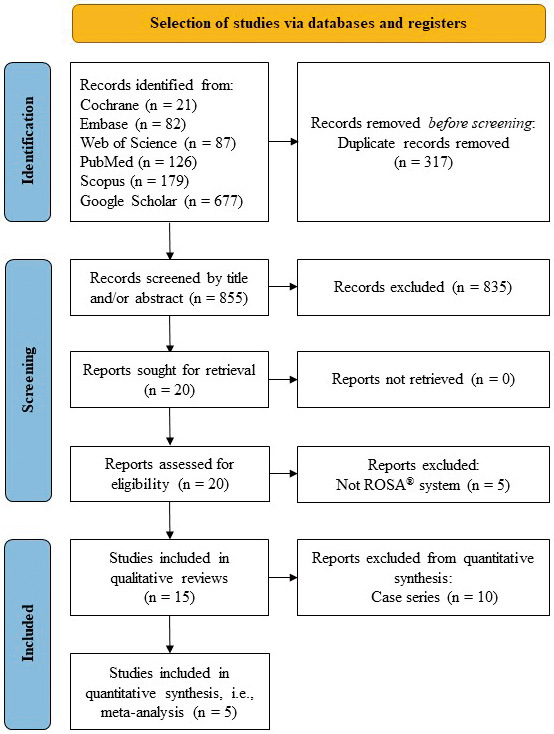
The aim of this study was to systematically review and meta-analyze the efficiency and safety of using the Robotic Stereotactic Assistance (ROSA®) device (Zimmer Biomet; Warsaw, IN, USA) for stereoelectroencephalography (SEEG) electrode implantation in patients with drug-resistant epilepsy. Based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, a literature search was carried out. Overall, 855 nonduplicate relevant articles were determined, and 15 of them were selected for analysis. The benefits of the ROSA® device use in terms of electrode placement accuracy, as well as operative time length, perioperative complications, and seizure outcomes, were evaluated. Studies that were included reported on a total of 11,257 SEEG electrode implantations. The limited number of comparative studies hindered the comprehensive evaluation of the electrode implantation accuracy. Compared with frame-based or navigation-assisted techniques, ROSA®-assisted SEEG electrode implantation provided significant benefits for reduction of both overall operative time (mean difference [MD], -63.45 min; 95% confidence interval [CI] from -88.73 to -38.17 min; P < 0.00001) and operative time per implanted electrode (MD, -8.79 min; 95% CI from -14.37 to -3.21 min; P = 0.002). No significant differences existed in perioperative complications and seizure outcomes after the application of the ROSA® device and other techniques for electrode implantation. To conclude, the available evidence shows that the ROSA® device is an effective and safe surgical tool for trajectory-guided SEEG electrode implantation in patients with drug-resistant epilepsy, offering benefits for saving operative time and neither increasing the risk of perioperative complications nor negatively impacting seizure outcomes.
Keywords: Robotic Stereotactic Assistance (ROSA®); depth electrode implantation; efficacy; epilepsy; stereoelectroencephalography.
Conflict of interest statement
Neither author has any actual or potential conflicts of interest related to this study. All Japan Neurosurgical Society (JNS) member authors (MC, SY, and YK) have registered online self-reported COI Disclosure Statement Forms via the JNS website.
Figures



Similar articles
-
Comparison of 2 Robotic Systems for Pediatric Stereoelectroencephalography Implantation.World Neurosurg. 2024 Feb;182:e486-e492. doi: 10.1016/j.wneu.2023.11.125. Epub 2023 Nov 30. World Neurosurg. 2024. PMID: 38042289
-
How can the accuracy of SEEG be increased?-an analysis of the accuracy of multilobe-spanning SEEG electrodes based on a frameless stereotactic robot-assisted system.Ann Palliat Med. 2021 Apr;10(4):3699-3705. doi: 10.21037/apm-20-2123. Epub 2021 Mar 10. Ann Palliat Med. 2021. PMID: 33691455
-
A Multivariate Approach to Quantifying Risk Factors Impacting Stereotactic Robotic-Guided Stereoelectroencephalography.Oper Neurosurg. 2025 Jun 1;28(6):824-831. doi: 10.1227/ons.0000000000001383. Epub 2024 Sep 27. Oper Neurosurg. 2025. PMID: 39329517
-
Robotic-Assisted Stereoelectroencephalography: A Systematic Review and Meta-Analysis of Safety, Outcomes, and Precision in Refractory Epilepsy Patients.Cureus. 2023 Oct 25;15(10):e47675. doi: 10.7759/cureus.47675. eCollection 2023 Oct. Cureus. 2023. PMID: 38021558 Free PMC article. Review.
-
Is the use of Stereotactic Electroencephalography Safe and Effective in Children? A Meta-Analysis of the use of Stereotactic Electroencephalography in Comparison to Subdural Grids for Invasive Epilepsy Monitoring in Pediatric Subjects.Neurosurgery. 2019 Jun 1;84(6):1190-1200. doi: 10.1093/neuros/nyy466. Neurosurgery. 2019. PMID: 30351382 Review.
References
-
- Beghi E: The epidemiology of epilepsy. Neuroepidemiology 54: 185-191, 2020 - PubMed
-
- Kalilani L, Sun X, Pelgrims B, Noack-Rink M, Villanueva V: The epidemiology of drug-resistant epilepsy: a systematic review and meta-analysis. Epilepsia 59: 2179-2193, 2018 - PubMed
-
- Rosenow F, Lüders H: Presurgical evaluation of epilepsy. Brain 124: 1683-1700, 2001 - PubMed
-
- Gonzalez-Martinez J, Bulacio J, Alexopoulos A, Jehi L, Bingaman W, Najm I: Stereoelectroencephalography in the “difficult to localize” refractory focal epilepsy: early experience from a North American epilepsy center. Epilepsia 54: 323-330, 2013 - PubMed