

Combined thoracoscopic and laparoscopic surgery for epiphrenic diverticulum with associated gastroesophageal reflux disease: a case report
- PMID: 38221572
- PMCID: PMC10788325
- DOI: 10.1186/s40792-024-01813-0
Combined thoracoscopic and laparoscopic surgery for epiphrenic diverticulum with associated gastroesophageal reflux disease: a case report
Abstract
Background: Surgery is indicated for symptomatic epiphrenic esophageal diverticula. Based on the features of a case, thoracoscopic or laparoscopic approaches may be used. Epiphrenic diverticula are often associated with esophageal motility disorders, but cases of reflux esophagitis have rarely been reported. In this report, we describe a case of an epiphrenic esophageal diverticulum with reflux esophagitis, which was successfully treated by thoracoscopic diverticulectomy and laparoscopic fundoplication.
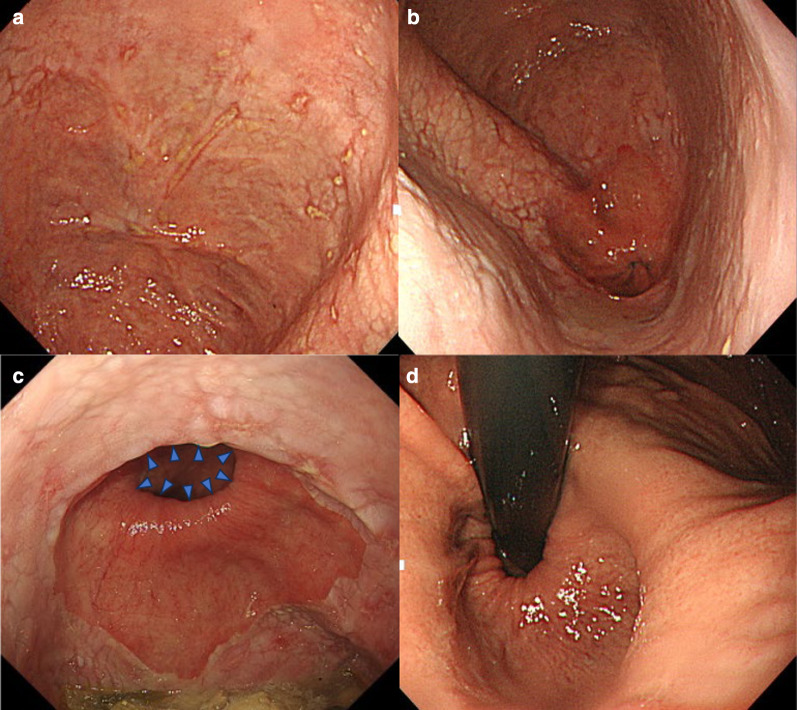
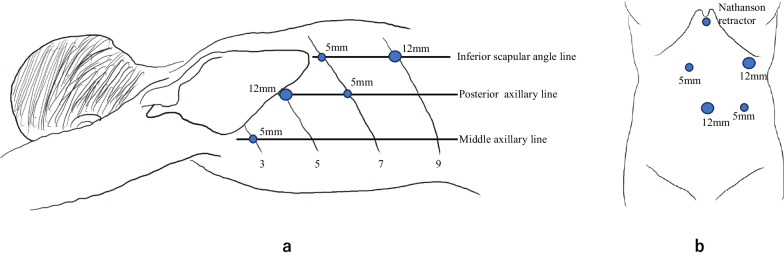
Case presentation: A 69-year-old man visited the hospital with a chief complaint of eructation and hiccup. Upper gastrointestinal endoscopy revealed a diverticulum in the left wall of the esophagus, which was 37-45 cm distal to the incisors. High-resolution manometry (HRM) showed no esophageal motility disorders. Due to the large size of the diverticulum, a thoracoscopic resection of the esophageal diverticulum was performed. Additionally, the patient had reflux esophagitis due to a hiatal hernia. The anti-reflux mechanism would be more impaired during the diverticulectomy; therefore, we decided that anti-reflux surgery should be performed simultaneously. Thoracoscopic esophageal diverticulectomy and laparoscopic Dor fundoplication were performed. The patient had an uncomplicated postoperative course and was discharged on the tenth operative day. He has been symptom-free without acid secretion inhibitors for 21 months after the surgery.
Conclusions: We described a rare case of a large epiphrenic diverticulum with reflux esophagitis. A good surgical outcome was achieved by thoracoscopic resection of the diverticulum and laparoscopic Dor fundoplication.
Keywords: Epiphrenic diverticulum; Reflux esophagitis; Thoracoscopic diverticulectomy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they do not have any competing interests regarding the publication of this article.
Figures




Similar articles
-
Laparoscopic Approach to Epiphrenic Diverticula Under Endoscopic Assistance: A Technical Report.J Laparoendosc Adv Surg Tech A. 2024 Feb;34(2):162-166. doi: 10.1089/lap.2023.0469. Epub 2023 Dec 18. J Laparoendosc Adv Surg Tech A. 2024. PMID: 38109227 Review.
-
Laparoscopic transhiatal surgery for an epiphrenic esophageal diverticulum derived from a jackhammer esophagus: a case report.Surg Case Rep. 2020 Jun 29;6(1):151. doi: 10.1186/s40792-020-00900-2. Surg Case Rep. 2020. PMID: 32601779 Free PMC article.
-
Laparoscopic transhiatal surgery based on high-resolution manometric evaluation of epiphrenic esophageal diverticulum.Clin J Gastroenterol. 2025 Feb;18(1):37-42. doi: 10.1007/s12328-024-02056-0. Epub 2024 Oct 30. Clin J Gastroenterol. 2025. PMID: 39477872
-
Esophageal manometric characteristics and outcomes for laparoscopic esophageal diverticulectomy, myotomy, and partial fundoplication for epiphrenic diverticula.Surg Endosc. 2009 Jun;23(6):1337-41. doi: 10.1007/s00464-008-0165-9. Epub 2008 Sep 24. Surg Endosc. 2009. PMID: 18813978
-
Optimal surgical approaches for esophageal epiphrenic diverticulum: literature review and our experience.Clin J Gastroenterol. 2023 Jun;16(3):317-324. doi: 10.1007/s12328-023-01765-2. Epub 2023 Feb 1. Clin J Gastroenterol. 2023. PMID: 36723767 Free PMC article. Review.
Cited by
-
Thoracoscopic Diverticulectomy for Epiphrenic Esophageal Diverticulum after Peroral Endoscopic Myotomy: A Report of Four Cases.Surg Case Rep. 2025;11(1):25-0065. doi: 10.70352/scrj.cr.25-0065. Epub 2025 Jun 20. Surg Case Rep. 2025. PMID: 40552008 Free PMC article.
References
LinkOut - more resources
Full Text Sources
