

A Case of Anterior Arytenoid Cartilage Dislocation During Nasal Tracheal Intubation Using an Indirect Video Laryngoscope
- PMID: 38221697
- PMCID: PMC11088197
- DOI: 10.2344/837325
A Case of Anterior Arytenoid Cartilage Dislocation During Nasal Tracheal Intubation Using an Indirect Video Laryngoscope
Abstract
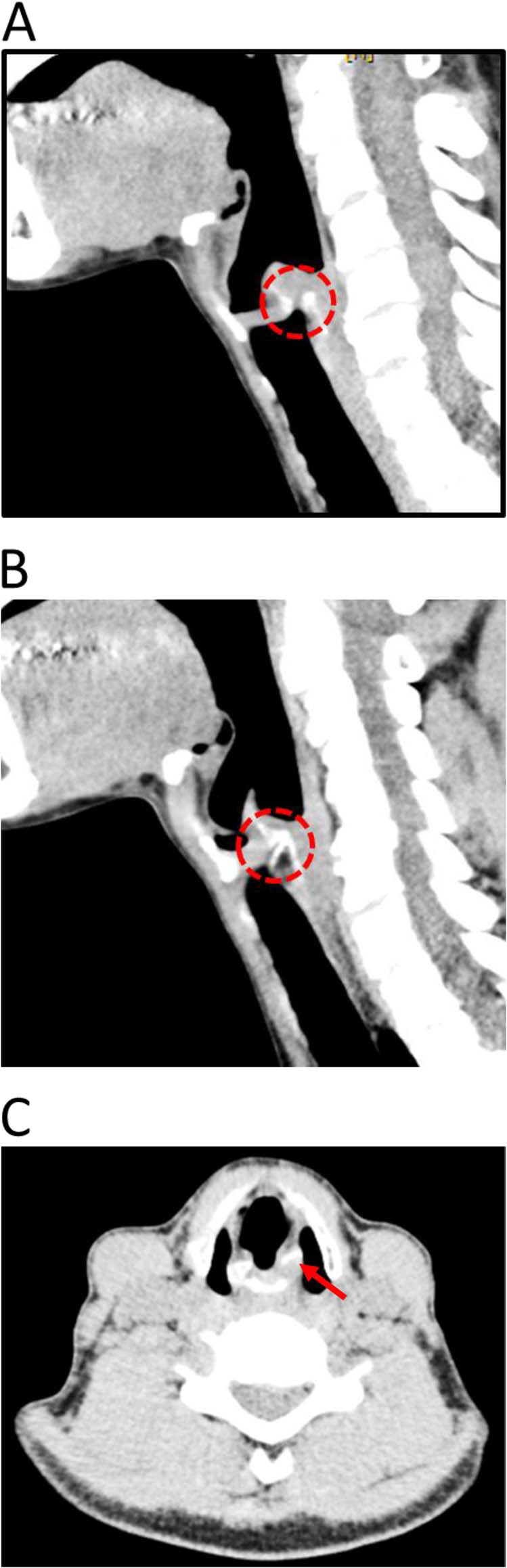
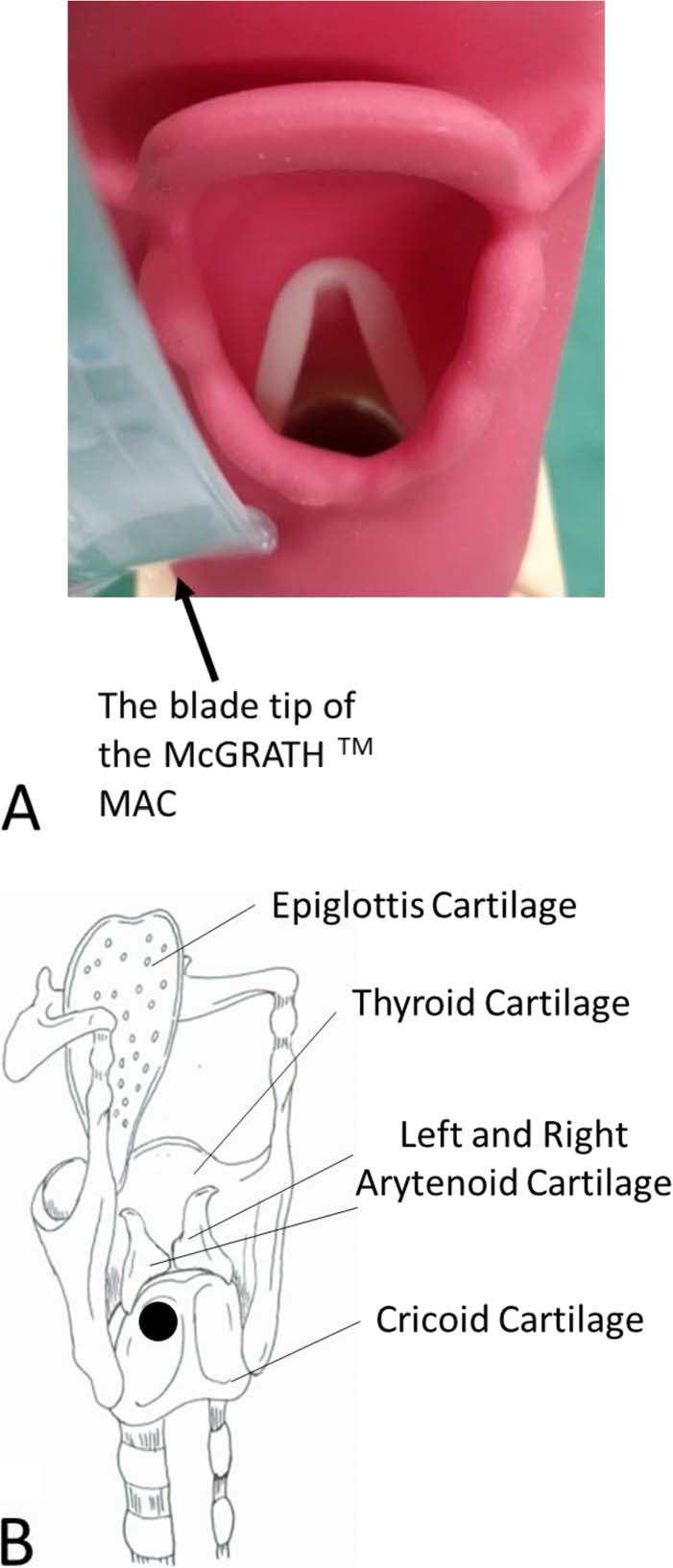
Arytenoid cartilage dislocation can occur as a complication of tracheal intubation and laryngeal trauma, but its occurrence with indirect video laryngoscopy has not been reported. This paper reports anterior arytenoid dislocation occurring after nasotracheal intubation performed under indirect laryngoscopy using a video laryngoscope (McGRATH MAC; Medtronic). The dislocation is presumed to have resulted from the laryngoscope blade being initially inserted too deeply and applying pressure to the posterior aspect of the left cricoarytenoid joint. This patient's anterior arytenoid dislocation was treated conservatively using speech therapy with resolution occurring approximately 40 days postoperatively. On the 74th day after surgery, fibroscopic examination confirmed recovery and healing of the dislocation. However, other types of arytenoid dislocations and laryngeal injuries may require alternative treatment. Early consultation with an otolaryngologist is recommended if arytenoid dislocation is suspected.
Keywords: Arytenoid cartilage dislocation; General anesthesia; Hoarseness; Indirect laryngoscopy; Tracheal intubation; Video laryngoscope.
© 2023 by the American Dental Society of Anesthesiology.
Figures
Similar articles
-
Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation.Cochrane Database Syst Rev. 2016 Nov 15;11(11):CD011136. doi: 10.1002/14651858.CD011136.pub2. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2022 Apr 4;4:CD011136. doi: 10.1002/14651858.CD011136.pub3. PMID: 27844477 Free PMC article. Updated.
-
Impact of universal use of the McGrath videolaryngoscope as the first option for all intubations in the operating room: The multicentre prospective before-after VIDEOLAR-SURGERY study protocol.Rev Esp Anestesiol Reanim (Engl Ed). 2025 Jan;72(1):101649. doi: 10.1016/j.redare.2024.101649. Epub 2024 Nov 12. Rev Esp Anestesiol Reanim (Engl Ed). 2025. PMID: 39542091
-
[Clinical report of hoding cricoarytenoid joint reduction with visual laryngoscope under intravenous anesthesia].Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2022 Sep 7;57(9):1095-1101. doi: 10.3760/cma.j.cn115330-20220221-00076. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2022. PMID: 36177564 Chinese.
-
Effect of head and neck positions on tracheal intubation using a McGRATH MAC video laryngoscope: A randomised, prospective study.Eur J Anaesthesiol. 2023 Aug 1;40(8):560-567. doi: 10.1097/EJA.0000000000001838. Epub 2023 Apr 13. Eur J Anaesthesiol. 2023. PMID: 37052067 Clinical Trial.
-
[Intubation trauma of the larynx--a literature review with special reference to arytenoid cartilage dislocation].Anasthesiol Intensivmed Notfallmed Schmerzther. 1996 Jun;31(5):281-7. doi: 10.1055/s-2007-995921. Anasthesiol Intensivmed Notfallmed Schmerzther. 1996. PMID: 8767240 Review. German.
References
-
- Abe K,, Nishino H,, Makino N. Fiberscopic reduction under local anesthesia for anterior arytenoid cartilage dislocation (in Japanese) Nippon Jibiinkoka Gakkai Kaiho 2007. 110 13–19 - PubMed
-
- Szigeti CL,, Baeuerle JJ,, Mongan PD. Arytenoid dislocation with lighted stylet intubation; case report and retrospective review Anesth Analg 1994. 78 185–186 - PubMed
-
- Close LG,, Merkel M,, Watson B,, Schaefer SD. Cricoarytenoid subluxation, computed tomography, and electromyography findings Head Neck Surg 1987. 9 (4) 341–348 - PubMed
-
- Quick CA,, Merwin GE. Arytenoid dislocation Arch Otolaryngol 1978. 104 267–270 - PubMed
-
- Sataloff FP,, Bough D,, Spiegel JR. Arytenoid dislocation: diagnosis and treatment Laryngoscope 1994. 104 1353–1361 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
