

Duodenojejunostomy treatment of groove pancreatitis-induced stenosis and obstruction of the horizontal duodenum: A case report
- PMID: 38222014
- PMCID: PMC10784829
- DOI: 10.4240/wjgs.v15.i12.2945
Duodenojejunostomy treatment of groove pancreatitis-induced stenosis and obstruction of the horizontal duodenum: A case report
Abstract
Background: Groove pancreatitis (GP) is a rare condition affecting the pancreatic groove region within the dorsal-cranial part of the pancreatic head, duodenum, and common bile duct. As a rare form of chronic pancreatitis, GP poses a diagnostic and therapeutic challenge for clinicians. GP is frequently misdiagnosed or not considered; thus, the diagnosis is often delayed by weeks or months. The treatment of GP is complicated and often requires surgical intervention, especially pancreatoduodenectomy.
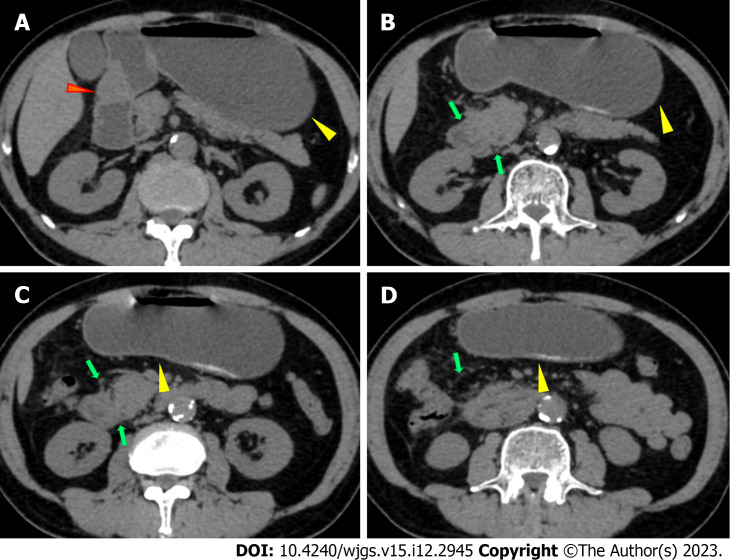
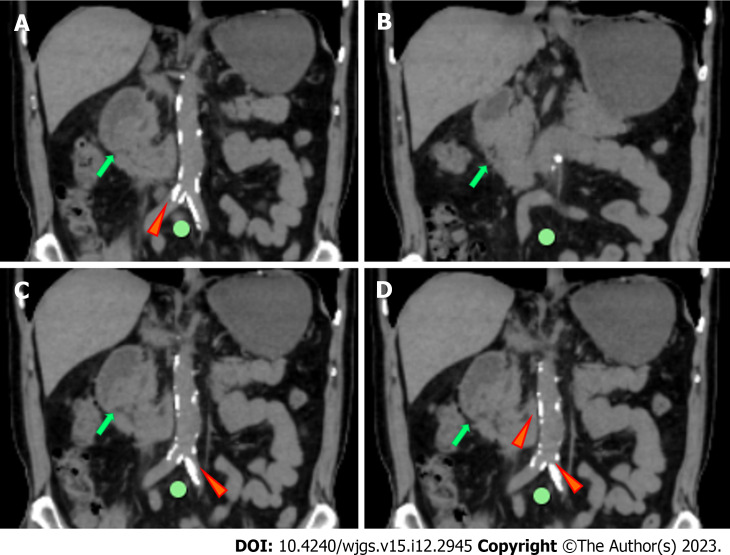
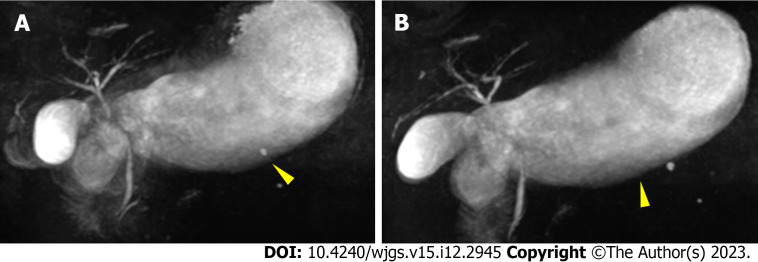
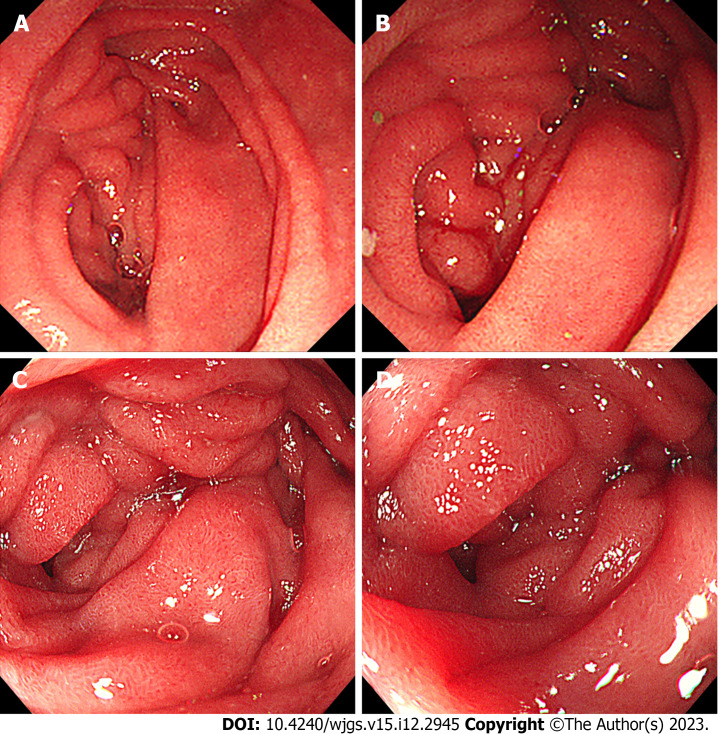
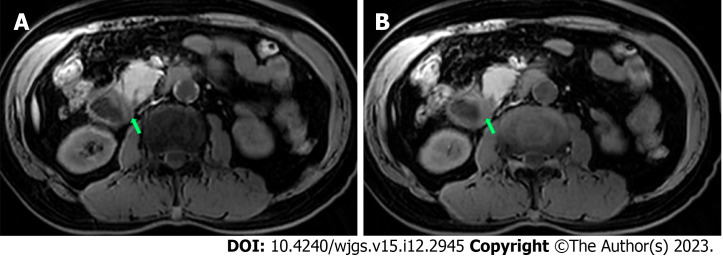
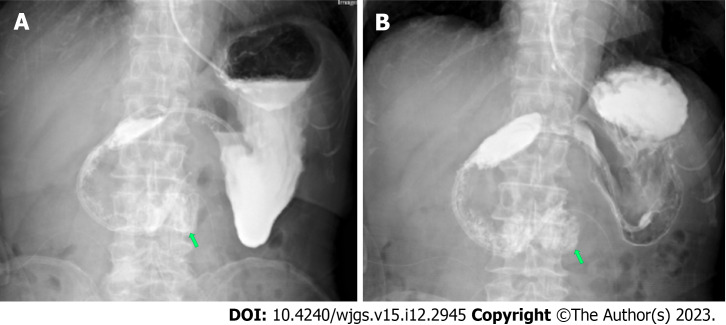
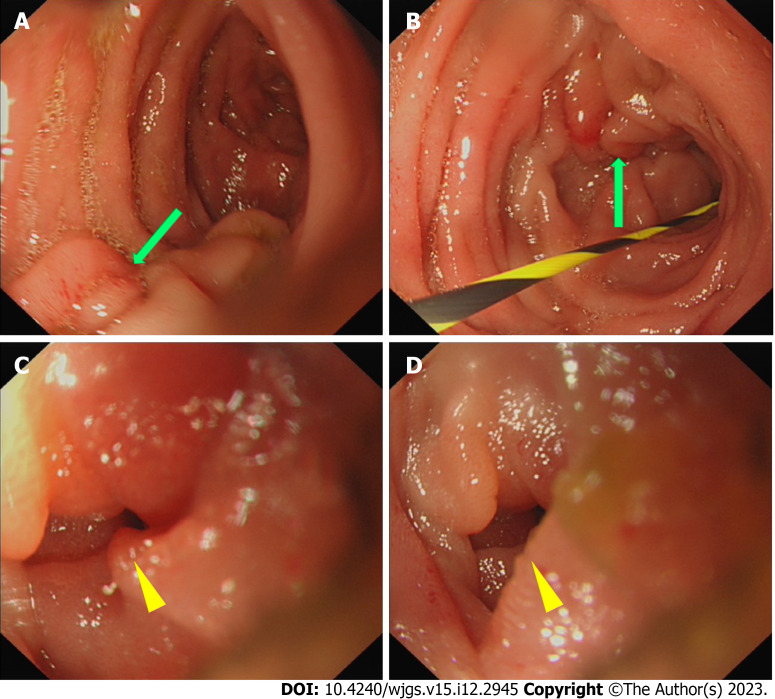
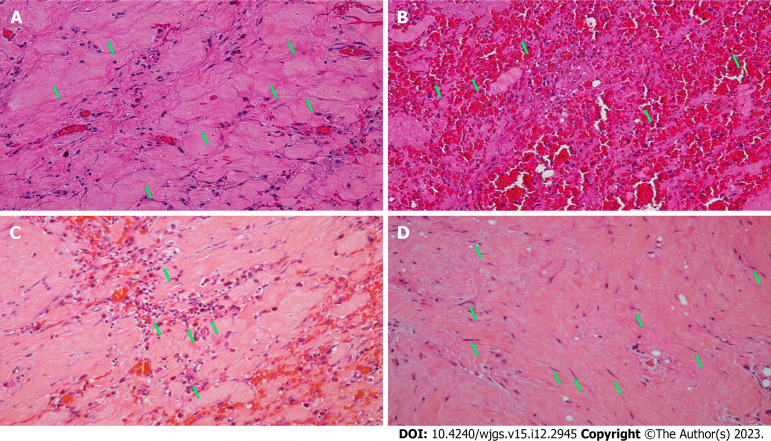
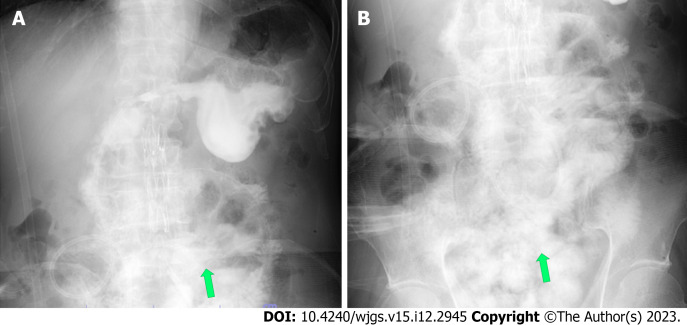
Case summary: A 66-year-old man with a history of long-term drinking was admitted to the gastroenterology department of our hospital, complaining of vomiting and acid reflux. Upper gastrointestinal endoscopy showed luminal stenosis in the descending part of the duodenum. Abdominal computed tomography showed slight exudation in the descending and horizontal parts of the duodenum with broadening of the groove region, indicating local pancreatitis. The symptoms of intestinal obstruction were not relieved with conservative therapy, and insertion of an enteral feeding tube was not successful. Exploratory laparoscopy was performed and revealed a hard mass with scarring in the horizontal part of the duodenum and stenosis. Intraoperative frozen section analysis showed no evidence of malignancy, and side-to-side duodenojejunostomy was performed. Routine pathologic examination showed massive proliferation of fibrous tissue, hyaline change, and the proliferation of spindle cells. Based on the radiologic and pathologic characteristics, a diagnosis of GP was made. The patient presented with anastomotic obstruction postoperatively and took a long time to recover, requiring supportive therapy.
Conclusion: GP often involves the descending and horizontal parts of the duodenum and causes duodenal stenosis, impaired duodenal motility, and gastric emptying due to fibrosis.
Keywords: Case report; Duodenal obstruction; Duodenal stenosis; Duodenojejunostomy; Groove pancreatitis.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Complete duodenal obstruction induced by groove pancreatitis: A case report.World J Clin Cases. 2019 Dec 6;7(23):4106-4110. doi: 10.12998/wjcc.v7.i23.4106. World J Clin Cases. 2019. PMID: 31832415 Free PMC article.
-
Pancreatoduodenectomy for paraduodenal pancreatitis: a diagnostic and therapeutic challenge.J Int Med Res. 2020 Nov;48(11):300060520972576. doi: 10.1177/0300060520972576. J Int Med Res. 2020. PMID: 33213250 Free PMC article.
-
Groove pancreatitis.Dig Surg. 2010;27(2):149-52. doi: 10.1159/000289099. Epub 2010 Jun 10. Dig Surg. 2010. PMID: 20551662 Review.
-
Acute pancreatitis associated with duodenal obstruction induced by groove pancreatitis: A case report.Medicine (Baltimore). 2021 Jun 4;100(22):e26139. doi: 10.1097/MD.0000000000026139. Medicine (Baltimore). 2021. PMID: 34087866 Free PMC article.
-
Groove pancreatitis: a case report and review of literature.JOP. 2007 Sep 7;8(5):592-7. JOP. 2007. PMID: 17873465 Review.
Cited by
-
Pancreatoduodenectomy and surgical treatment of groove pancreatitis.Arq Bras Cir Dig. 2025 Aug 29;38:e1895. doi: 10.1590/0102-67202025000026e1895. eCollection 2025. Arq Bras Cir Dig. 2025. PMID: 40900574 Free PMC article. Review.
References
-
- Manzelli A, Petrou A, Lazzaro A, Brennan N, Soonawalla Z, Friend P. Groove pancreatitis. A mini-series report and review of the literature. JOP. 2011;12:230–233. - PubMed
-
- Potet F, Duclert N. Cystic dystrophy on aberrant pancreas of the duodenal wall. Arch Fr Mal App Dig. 1970;59:223–238. - PubMed
-
- Kager LM, Lekkerkerker SJ, Arvanitakis M, Delhaye M, Fockens P, Boermeester MA, van Hooft JE, Besselink MG. Outcomes After Conservative, Endoscopic, and Surgical Treatment of Groove Pancreatitis: A Systematic Review. J Clin Gastroenterol. 2017;51:749–754. - PubMed
-
- Stolte M, Weiss W, Volkholz H, Rösch W. A special form of segmental pancreatitis: "groove pancreatitis". Hepatogastroenterology. 1982;29:198–208. - PubMed
-
- Adsay NV, Zamboni G. Paraduodenal pancreatitis: a clinico-pathologically distinct entity unifying "cystic dystrophy of heterotopic pancreas", "para-duodenal wall cyst", and "groove pancreatitis". Semin Diagn Pathol. 2004;21:247–254. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
