

Balancing risks of recurrent venous thromboembolism and bleeding with extended anticoagulation: a decision analysis
- PMID: 38222076
- PMCID: PMC10784302
- DOI: 10.1016/j.rpth.2023.102274
Balancing risks of recurrent venous thromboembolism and bleeding with extended anticoagulation: a decision analysis
Abstract
Background: A decision to stop or continue anticoagulation after 3 months of anticoagulation for venous thromboembolism (VTE) should be made by weighing individual risks of recurrence and bleeding.
Objectives: To determine the optimal ratio of recurrence risk reduction to increase the risk of bleeding in terms of maximizing quality-adjusted life years (QALYs) gained.
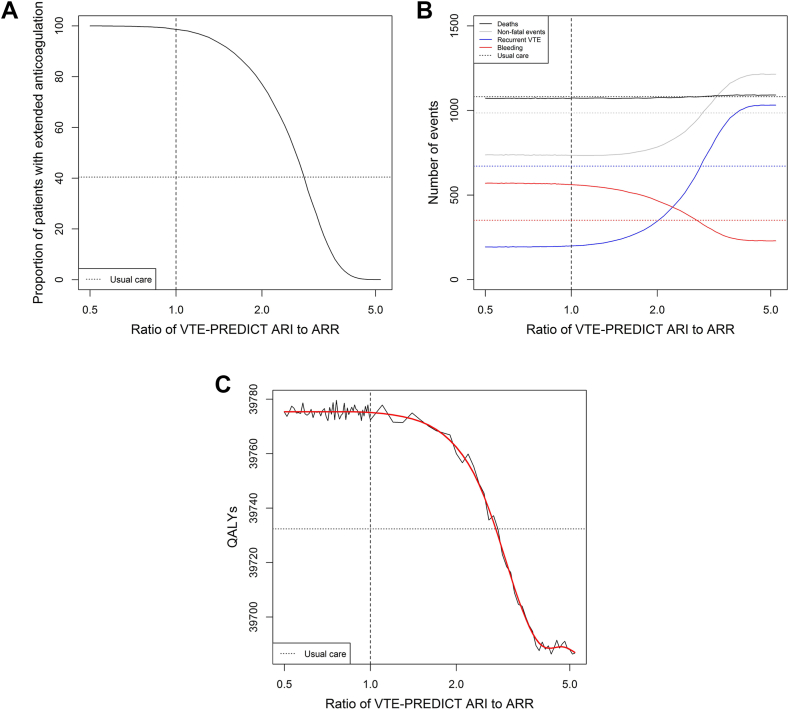
Methods: Using a microsimulation model, outcomes within 5 years were simulated after assigning extended treatment if absolute recurrence risk reduction outweighed absolute increase in clinically relevant bleeding risk (International Society on Thrombosis and Haemostasis definition), weighted by a certain ratio. Data were simulated based on the Bleeding Risk Study, a prospective cohort including patients after ≥3 months of anticoagulation for unprovoked VTE or provoked VTE with history of VTE. The VTE-PREDICT risk score was used to estimate 5-year risks of recurrent VTE and clinically relevant bleeding.
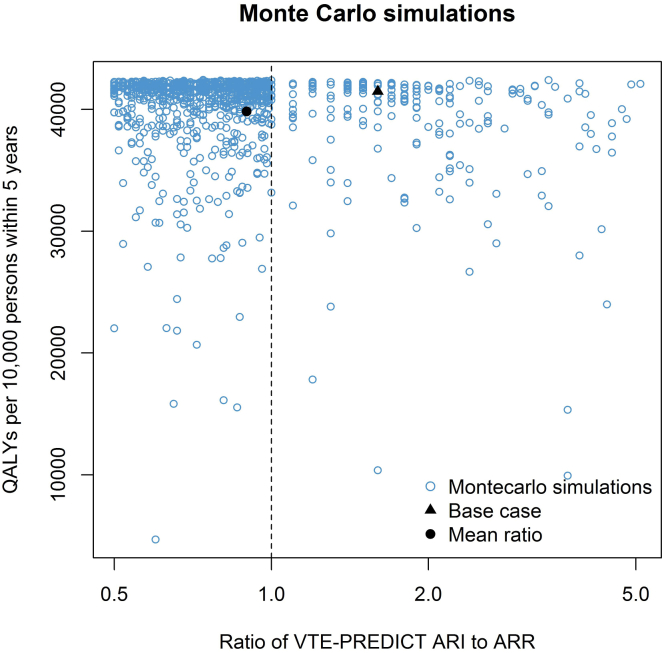
Results: Among 10,000 individuals (mean age, 60.2 years, 36% female), the ratio of 0.90 (95% CI, 0.51-3.40; ie, bleeding is considered 0.90 the severity of recurrent VTE), with 99% of patients assigned extended anticoagulation, was considered optimal and resulted in 93 (95% CI, -23 to 203) additional QALYs compared with the least favorable ratio (5.10, 0% extended anticoagulation). At the optimal ratio, treatment based on VTE-PREDICT yielded 44 (95% CI, -69 to 157) additional QALYs versus standard of care.
Conclusion: With the current evidence, the optimal ratio between relevant bleeding risk and absolute recurrence risk reduction remains uncertain. Our results confirm that clinical equipoise exists regarding the decision to stop or continue anticoagulation after initial VTE treatment, emphasizing the importance of shared decision-making.
Keywords: anticoagulation; bleeding; quality-adjusted life years; risk; venous thromboembolism.
© 2023 The Authors.
Figures

Similar articles
-
Recurrent venous thromboembolism and bleeding with extended anticoagulation: the VTE-PREDICT risk score.Eur Heart J. 2023 Apr 7;44(14):1231-1244. doi: 10.1093/eurheartj/ehac776. Eur Heart J. 2023. PMID: 36648242 Free PMC article.
-
Indefinite Anticoagulant Therapy for First Unprovoked Venous Thromboembolism : A Cost-Effectiveness Study.Ann Intern Med. 2023 Jul;176(7):949-960. doi: 10.7326/M22-3559. Epub 2023 Jun 27. Ann Intern Med. 2023. PMID: 37364263
-
Safety and Efficacy of Rivaroxaban for Extended-Phase Anticoagulation of Patients with Unprovoked or Recurrent Venous Thromboembolism: Real-Life Data from the MAC Project.Life (Basel). 2022 Oct 20;12(10):1657. doi: 10.3390/life12101657. Life (Basel). 2022. PMID: 36295091 Free PMC article.
-
Direct oral anticoagulants for extended treatment of venous thromboembolism: insights from the EINSTEIN CHOICE study.Blood Transfus. 2020 Jan;18(1):49-57. doi: 10.2450/2019.0265-18. Epub 2019 Apr 30. Blood Transfus. 2020. PMID: 31184579 Free PMC article. Review.
-
Long-term risk of recurrent venous thromboembolism among patients receiving extended oral anticoagulant therapy for first unprovoked venous thromboembolism: A systematic review and meta-analysis.J Thromb Haemost. 2021 Nov;19(11):2801-2813. doi: 10.1111/jth.15491. Epub 2021 Aug 22. J Thromb Haemost. 2021. PMID: 34379859
Cited by
-
Balancing the risks of recurrent venous thromboembolism and bleeding with extended anticoagulation: oh, for a crystal ball!Res Pract Thromb Haemost. 2024 Jan 18;8(1):102316. doi: 10.1016/j.rpth.2024.102316. eCollection 2024 Jan. Res Pract Thromb Haemost. 2024. PMID: 38356852 Free PMC article. No abstract available.
References
-
- Konstantinides S.V., Meyer G., Becattini C., Bueno H., Geersing G.-J., Harjola V.-P., et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) Eur Heart J. 2020;41:543–603. - PubMed
-
- Stevens S.M., Woller S.C., Baumann Kreuziger L., Bounameaux H., Doerschug K., Geersing G.-J., et al. Antithrombotic therapy for VTE disease: second update of the CHEST guideline and expert panel report. Chest. 2021;160:2247–2259. - PubMed
-
- Khan F., Rahman A., Carrier M., Kearon C., Weitz J.I., Schulman S., et al. Long term risk of symptomatic recurrent venous thromboembolism after discontinuation of anticoagulant treatment for first unprovoked venous thromboembolism event: systematic review and meta-analysis. BMJ. 2019;366:l4363. doi: 10.1136/bmj.l4363. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
