

Cardiac magnetic resonance imaging detection of intramyocardial hemorrhage in patients with ST-elevated myocardial infarction: comparison between susceptibility-weighted imaging and T1/T2 mapping techniques
- PMID: 38223054
- PMCID: PMC10784041
- DOI: 10.21037/qims-23-591
Cardiac magnetic resonance imaging detection of intramyocardial hemorrhage in patients with ST-elevated myocardial infarction: comparison between susceptibility-weighted imaging and T1/T2 mapping techniques
Abstract
Background: Susceptibility-weighted imaging (SWI) and T1/T2 mapping can be used to detect reperfusion intramyocardial hemorrhage (IMH) in ST-segment elevation myocardial infarction (STEMI) patients. However, the sensitivity and accuracy of the SWI and T1/T2 mapping sequences were not systematically compared. The study aimed to evaluate image quality and diagnostic performance of SWI in patients with IMH, compared with T1/T2 mapping.
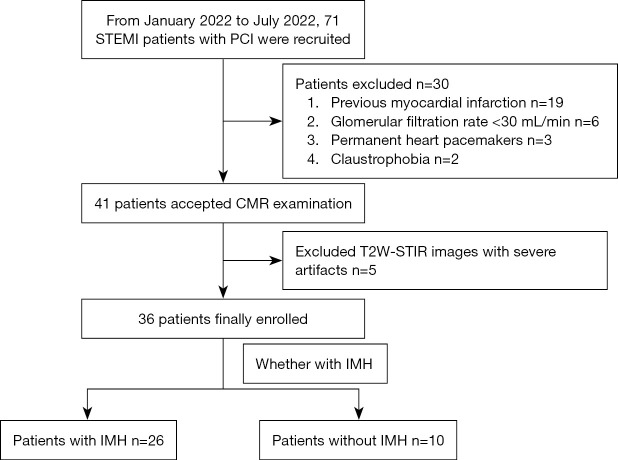
Methods: A prospective study was conducted on consecutive acute STEMI patients who were recruited from January to July 2022. Within 2-6 days after reperfusion treatment, all patients underwent a 3T cardiac magnetic resonance (CMR) examination, including T2-weighted short-tau inversion recovery (T2W-STIR), T1/T2 mapping, and SWI. A total of 36 patients [age, 56.50±17.25 years; males, 83.33% (30/36)] were enrolled. The relative infarct-remote myocardium signal intensity ratio (SIinfarct-remote) and contrast-to-noise ratio (CNR) were calculated for each patient on T1/T2 mapping and SWI, and the difference between relative signal intensity-to-noise ratio (rSNR) in the IMH (rSNRIMH) was measured for IMH patients on T1/T2 mapping and SWI. SIinfarct-remote, CNR, and rSNRIMH were compared among the three sequences. Receiver operating characteristic (ROC) analyses were used to evaluate the diagnostic performance of three sequences by SIinfarct-remote and visual assessment.
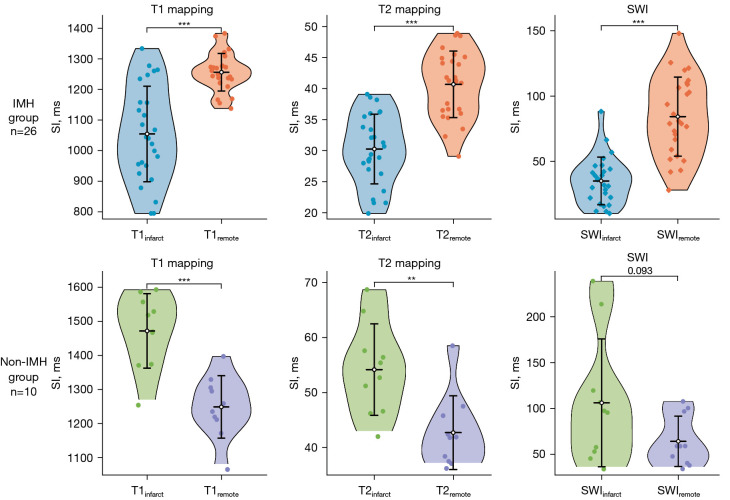
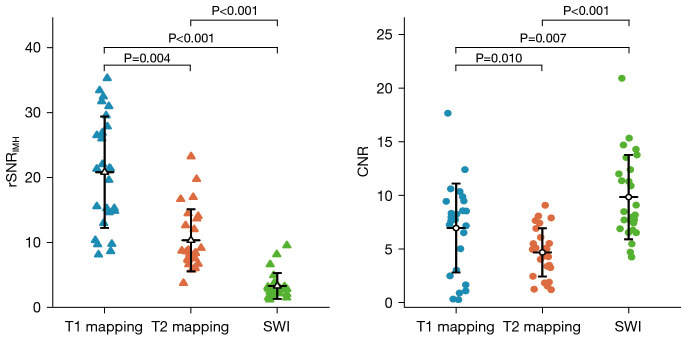
Results: A total of 26 (72.22%) patients had IMH. Quantitatively, the SIinfarct-remote of three sequences had excellent diagnostic performance for detecting IMH [SWI area under the curve (AUC) =1.000, 95% confidence interval (CI): 1.000-1.000 vs. T1 mapping AUC =0.954, 95% CI: 0.885-1.000 vs. T2 mapping AUC =0.985, 95% CI: 0.955-1.000; SWI vs. T1 mapping, P=0.300; SWI vs. T2 mapping, P=0.188; T1 mapping vs. T2 mapping, P=0.302). Qualitatively, three sequences had similar performance on detecting IMH (SWI AUC =0.895, 95% CI: 0.784-1.000; T1 mapping AUC =0.835, 95% CI: 0.711-0.958; and T2 mapping AUC =0.855, 95% CI: 0.735-0.974; SWI vs. T1 mapping, P=0.172; SWI vs. T2 mapping, P=0.317; T1 mapping vs. T2 mapping, P=0.710). The rSNRIMH was highest in T1 mapping, followed by T2 mapping and SWI, but SWI had the highest CNR.
Conclusions: SWI, as well as T1/T2 mapping, is a feasible and accurate approach for clinical diagnosis of IMH with excellent performance.
Keywords: Susceptibility-weighted imaging (SWI); T1 mapping; T2 mapping; cardiac magnetic resonance (CMR); intramyocardial hemorrhage (IMH).
2024 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-23-591/coif). X.T. and X.Z. are current employees of Bayer Healthcare and Siemens Healthineers, respectively. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Head-to-head comparison of multiple cardiovascular magnetic resonance techniques for the detection and quantification of intramyocardial haemorrhage in patients with ST-elevation myocardial infarction.Eur Radiol. 2021 Mar;31(3):1245-1256. doi: 10.1007/s00330-020-07254-1. Epub 2020 Sep 14. Eur Radiol. 2021. PMID: 32929640 Free PMC article.
-
Diagnostic performance of T1 and T2 mapping to detect intramyocardial hemorrhage in reperfused ST-segment elevation myocardial infarction (STEMI) patients.J Magn Reson Imaging. 2017 Sep;46(3):877-886. doi: 10.1002/jmri.25638. Epub 2017 Feb 15. J Magn Reson Imaging. 2017. PMID: 28199043 Free PMC article.
-
Assessment of intramyocardial hemorrhage by T1-weighted cardiovascular magnetic resonance in reperfused acute myocardial infarction.J Cardiovasc Magn Reson. 2012 Aug 30;14(1):59. doi: 10.1186/1532-429X-14-59. J Cardiovasc Magn Reson. 2012. PMID: 22935462 Free PMC article.
-
Cardiac MRI to Visualize Myocardial Damage after ST-Segment Elevation Myocardial Infarction: A Review of Its Histologic Validation.Radiology. 2021 Oct;301(1):4-18. doi: 10.1148/radiol.2021204265. Epub 2021 Aug 24. Radiology. 2021. PMID: 34427461 Review.
-
Impact of Intramyocardial Hemorrhage on Clinical Outcomes in ST-Elevation Myocardial Infarction: A Systematic Review and Meta-analysis.J Soc Cardiovasc Angiogr Interv. 2022 Aug 26;1(6):100444. doi: 10.1016/j.jscai.2022.100444. eCollection 2022 Nov-Dec. J Soc Cardiovasc Angiogr Interv. 2022. PMID: 39132339 Free PMC article. Review.
Cited by
-
Application of non-invasive imaging in myocardial infarction: a bibliometric analysis from January 2003 to December 2022.Quant Imaging Med Surg. 2025 Jul 1;15(7):6340-6359. doi: 10.21037/qims-24-878. Epub 2025 Jun 30. Quant Imaging Med Surg. 2025. PMID: 40727351 Free PMC article.
References
-
- Ghugre NR, Pop M, Thomas R, Newbigging S, Qi X, Barry J, Strauss BH, Wright GA. Hemorrhage promotes inflammation and myocardial damage following acute myocardial infarction: insights from a novel preclinical model and cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2017;19:50. 10.1186/s12968-017-0361-7 - DOI - PMC - PubMed
-
- Ferré-Vallverdú M, Sánchez-Lacuesta E, Plaza-López D, Díez-Gil JL, Sepúlveda-Sanchis P, Gil-Cayuela C, Maceira-Gonzalez A, Miró-Palau V, Montero-Argudo A, Martínez-Dolz L, Igual-Muñoz B. Prognostic value and clinical predictors of intramyocardial hemorrhage measured by CMR T2* sequences in STEMI. Int J Cardiovasc Imaging 2021;37:1735-44. 10.1007/s10554-020-02142-7 - DOI - PubMed
LinkOut - more resources
Full Text Sources