

Improved heart function and cardiac remodelling following sacubitril/valsartan in acute coronary syndrome with HF
- PMID: 38224955
- PMCID: PMC10966256
- DOI: 10.1002/ehf2.14646
Improved heart function and cardiac remodelling following sacubitril/valsartan in acute coronary syndrome with HF
Abstract
Aims: This study sought to assess the effect of treatment of sacubitril/valsartan (S/V) on improving cardiac function and reversing cardiac remodelling in patients with acute coronary syndrome (ACS) complicated with heart failure with reduced ejection fraction after percutaneous coronary intervention (PCI).
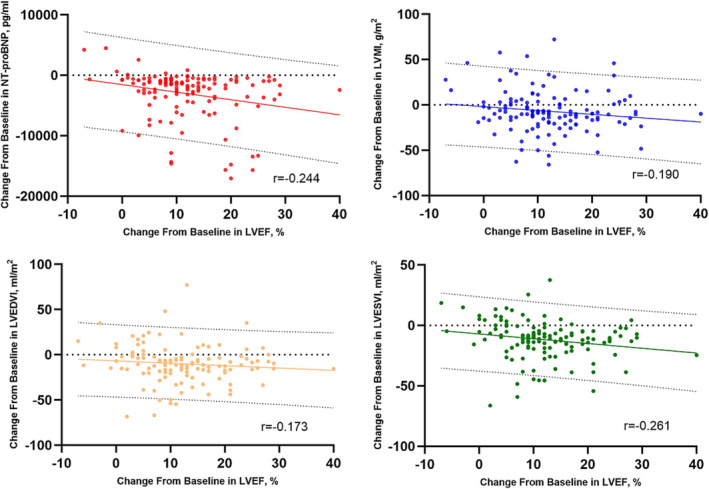
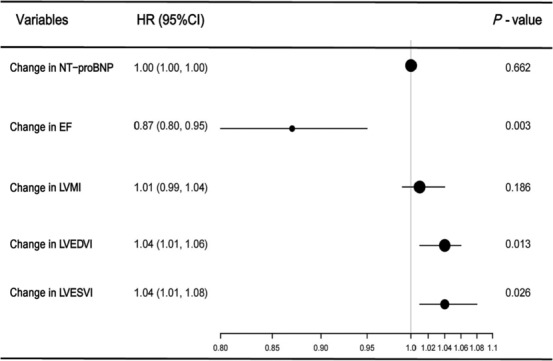
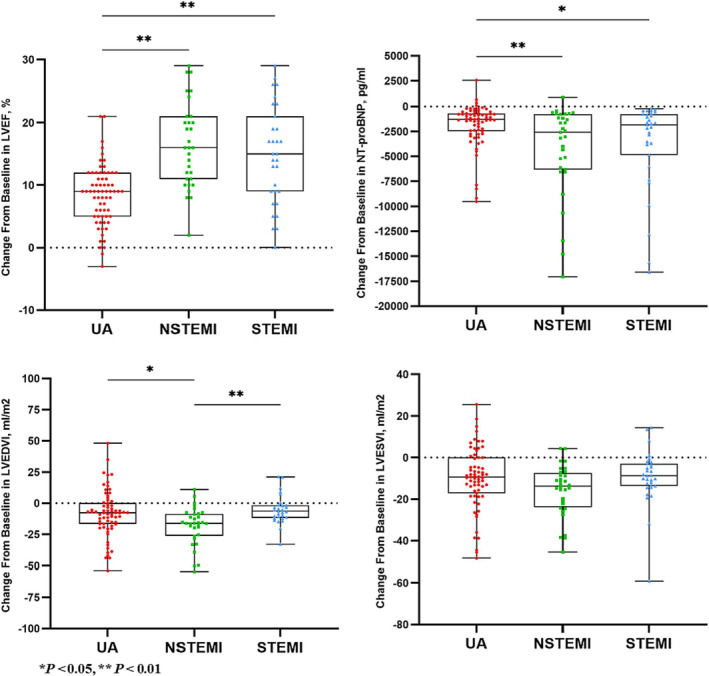
Methods and results: We enrolled 275 ACS patients with reduced left ventricular ejection fraction after PCI. The patients were divided into the routine and S/V groups according to the treatment drugs. The symptoms, N-terminal pro-brain natriuretic peptide (NT-proBNP) concentrations, echocardiographic parameters [left ventricular ejection fraction (LVEF), left ventricular mass index (LVMI), left ventricular end-diastolic volume index (LVEDVI), and left ventricular end-systolic volume index (LVESVI)], major adverse cardiac events (MACEs), and adverse reactions were recorded at baseline and 6 months after treatment when a clinical follow-up was performed. The S/V group was further divided into prespecified subgroups including unstable angina (UA) group, non-ST-elevation myocardial infarction (NSTEMI) group, and ST-elevation myocardial infarction (STEMI) group according to the type of ACS. We analysed the changes in LVEF, LVMI, LVEDVI, LVESVI, and NT-proBNP in both groups and evaluated the correlation between the changes in the above variables (ΔLVEF, ΔLVMI, ΔLVEDVI, ΔLVESVI, and ΔNT-proBNP). Cox regression model was used to assess the independent risk factors of MACE. Prespecified subgroup analyses were also conducted. Compared with baseline, LVEF increased significantly (P < 0.05), NT-proBNP, LVMI, and LVESVI decreased significantly in both groups after 6 months (P < 0.05), and LVEDVI decreased significantly in the S/V group (P = 0.001). In the S/V group, ΔLVEF (t = -2.745, P = 0.006), ΔNT-proBNP (P = 0.009), ΔLVEDVI (t = 4.203, P = 0.001), and ΔLVESVI (t = 3.907, P = 0.001) were significantly improved than those in the routine group. In the S/V group, ΔLVEF was negatively correlated with ΔNT-proBNP (r = -0.244, P = 0.004), ΔLVMI (r = -0.190, P = 0.028), ΔLVEDVI (r = -0.173, P = 0.045), and ΔLVESVI (r = -0.261, P = 0.002). In Cox regression model analysis, ΔLVEF {hazard ratio [HR] = 0.87 [95% confidence interval (CI) 0.80-0.95], P = 0.003}, ΔLVEDVI [HR = 1.04 (95% CI 1.01-1.06), P = 0.013], and ΔLVESVI [HR = 1.04 (95% CI 1.01-1.08), P = 0.026] were independent risk factors for MACE. Subgroup analysis showed that ΔLVEF (t = 6.290, P = 0.001), ΔLVEDVI (t = 2.581, P = 0.011), and ΔNT-proBNP (P = 0.019) in the NSTEMI group were significantly improved than those in the UA group, ΔLVEDVI in the NSTEMI group was significantly better than that in the STEMI group (t = -3.365, P = 0.001), and ΔLVEF in the STEMI group was significantly better than that in the UA group (t = -3.928, P = 0.001). There was a significant difference in the survival probability without MACE among the three groups in the analysis of the Kaplan-Meier curve (P = 0.042). The incidence of MACE in the UA group was significantly higher than that in the NSTEMI group (32.4% vs. 6.3%, P = 0.004).
Conclusions: The cardiac function is improved and cardiac remodelling is reversed significantly after treatment of S/V in ACS patients with reduced left ventricular ejection fraction after PCI, and the improvement is more obvious than the routine group. There is a significant negative correlation between the change in LVEF and the changes in NT-proBNP, LVMI, LVEDVI, and LVESVI. The increase of LVEF and the decrease of LVEDVI and LVESVI are protective factors to improve the prognosis. Patients with myocardial infarction and reduced left ventricular ejection fraction might benefit more from the initiation of S/V as first-line heart failure treatment after PCI.
Keywords: Acute coronary syndrome; Heart failure with reduced ejection fraction; Percutaneous coronary intervention; Sacubitril/valsartan.
© 2024 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Effect of sacubitril-valsartan on left ventricular remodeling in patients with acute myocardial infarction after primary percutaneous coronary intervention: a systematic review and meta-analysis.Front Pharmacol. 2024 May 28;15:1366035. doi: 10.3389/fphar.2024.1366035. eCollection 2024. Front Pharmacol. 2024. PMID: 38863978 Free PMC article.
-
Study on the application effect of bisoprolol combined with sacubitril valsartan sodium tablets in the cardiac rehabilitation of patients with acute myocardial infarction combined with left heart failure after percutaneous coronary intervention (PCI).Ann Palliat Med. 2021 May;10(5):5455-5461. doi: 10.21037/apm-21-877. Epub 2021 May 19. Ann Palliat Med. 2021. PMID: 34044572
-
[Effect of sacubitril/valsartan on cardiac function in heart failure rabbits with preserved ejection fraction].Zhonghua Xin Xue Guan Bing Za Zhi. 2019 Nov 24;47(11):887-893. doi: 10.3760/cma.j.issn.0253-3758.2019.11.007. Zhonghua Xin Xue Guan Bing Za Zhi. 2019. PMID: 31744278 Chinese.
-
Efficacy of early administration of sacubitril/valsartan after coronary artery revascularization in patients with acute myocardial infarction complicated by moderate-to-severe mitral regurgitation: a randomized controlled trial.Heart Vessels. 2024 Aug;39(8):673-686. doi: 10.1007/s00380-024-02398-2. Epub 2024 Apr 18. Heart Vessels. 2024. PMID: 38635062 Clinical Trial.
-
A systematic review and meta-analysis of sacubitril-valsartan in the treatment of ventricular remodeling in patients with heart failure after acute myocardial infarction.Front Cardiovasc Med. 2022 Oct 11;9:953948. doi: 10.3389/fcvm.2022.953948. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36304540 Free PMC article.
Cited by
-
Sacubitril/valsartan in a wide spectrum of heart failure patients (from mechanisms of action to outcomes in specific populations).Heart Fail Rev. 2025 Mar;30(2):387-405. doi: 10.1007/s10741-024-10471-1. Epub 2025 Jan 7. Heart Fail Rev. 2025. PMID: 39776087 Free PMC article. Review.
-
Efficacy of Sacubitril Valsartan sodium tablets in patients with heart failure combined with pulmonary infection and long-term recurrence rate.Am J Transl Res. 2024 Aug 15;16(8):3742-3750. doi: 10.62347/ESYO5136. eCollection 2024. Am J Transl Res. 2024. PMID: 39262724 Free PMC article.
-
Effect of sacubitril-valsartan on left ventricular remodeling in patients with acute myocardial infarction after primary percutaneous coronary intervention: a systematic review and meta-analysis.Front Pharmacol. 2024 May 28;15:1366035. doi: 10.3389/fphar.2024.1366035. eCollection 2024. Front Pharmacol. 2024. PMID: 38863978 Free PMC article.
-
Gut microbiota's role in heart failure.Heart Fail Rev. 2025 Jul 9. doi: 10.1007/s10741-025-10543-w. Online ahead of print. Heart Fail Rev. 2025. PMID: 40629225 Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
