

Dermatologist-like explainable AI enhances trust and confidence in diagnosing melanoma
- PMID: 38225244
- PMCID: PMC10789736
- DOI: 10.1038/s41467-023-43095-4
Dermatologist-like explainable AI enhances trust and confidence in diagnosing melanoma
Abstract
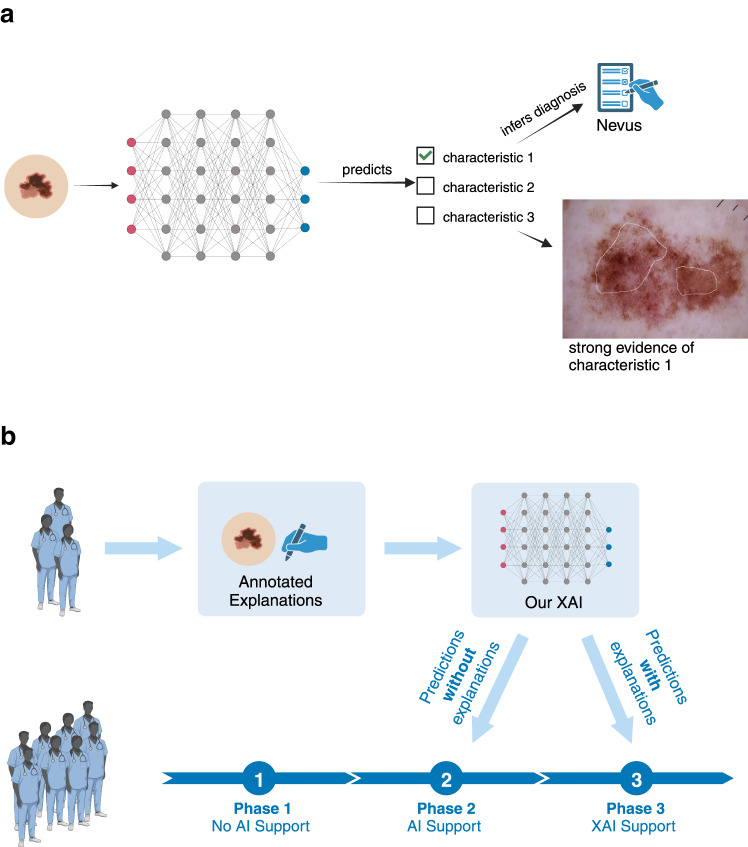
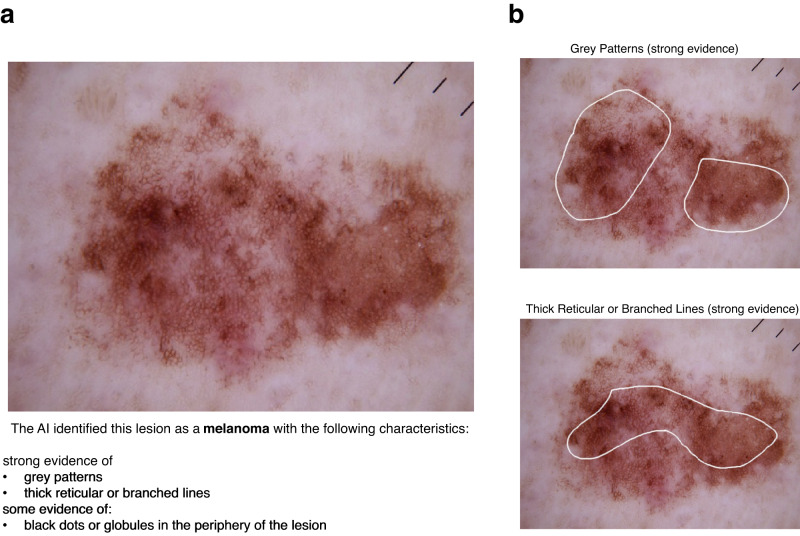
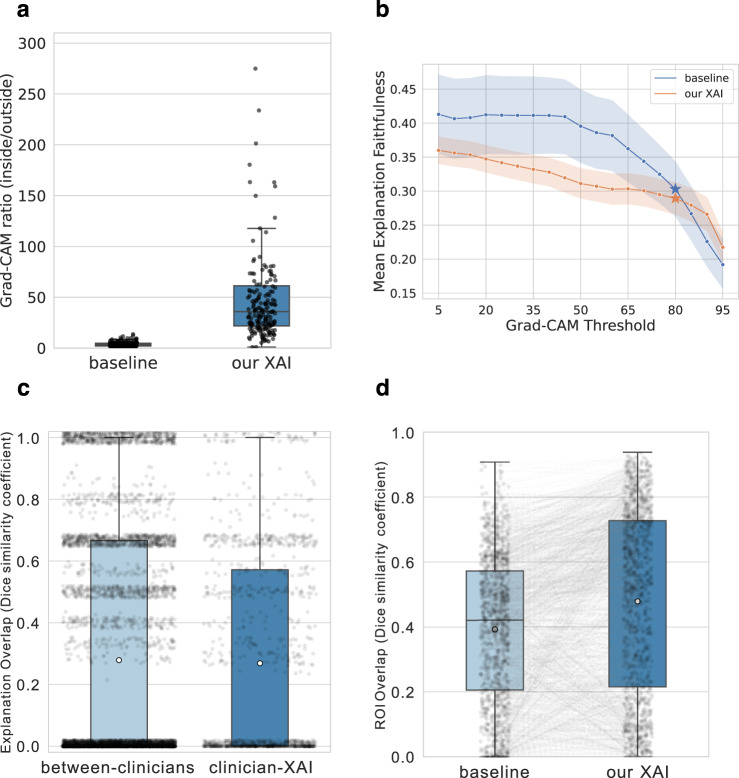
Artificial intelligence (AI) systems have been shown to help dermatologists diagnose melanoma more accurately, however they lack transparency, hindering user acceptance. Explainable AI (XAI) methods can help to increase transparency, yet often lack precise, domain-specific explanations. Moreover, the impact of XAI methods on dermatologists' decisions has not yet been evaluated. Building upon previous research, we introduce an XAI system that provides precise and domain-specific explanations alongside its differential diagnoses of melanomas and nevi. Through a three-phase study, we assess its impact on dermatologists' diagnostic accuracy, diagnostic confidence, and trust in the XAI-support. Our results show strong alignment between XAI and dermatologist explanations. We also show that dermatologists' confidence in their diagnoses, and their trust in the support system significantly increase with XAI compared to conventional AI. This study highlights dermatologists' willingness to adopt such XAI systems, promoting future use in the clinic.
© 2024. The Author(s).
Conflict of interest statement
PT reports grants from Lilly, consulting fees from Silverchair, lecture honoraria from Lilly, FotoFinder and Novartis, outside of the present publication. TJB owns a company that develops mobile apps (Smart Health Heidelberg GmbH, Heidelberg, Germany), outside of the scope of the submitted work. WS received travel support for participation in congresses and / or (speaker) honoraria as well as research grants from medi GmbH Bayreuth, Abbvie, Almirall, Amgen, Bristol-Myers Squibb, Celgene, GSK, Janssen, LEO Pharma, Lilly, MSD, Novartis, Pfizer, Roche, Sanofi Genzyme, and UCB outside of the present publication. MLV received travel support for participation in congresses and / or (speaker) honoraria as well as research grants from Abbvie, Almirall, Amgen, Bristol-Myers Squibb, Celgene, Janssen, Kyowa Kirin, LEO Pharma, Lilly, MSD, Novartis, Pfizer, Roche, Sanofi Genzyme, and UCB outside of the present publication. BS is on the advisory board or has received honoraria from Immunocore, Almirall, Pfizer, Sanofi, Novartis, Roche, BMS and MSD, research funding from Novartis and Pierre Fabre Pharmaceuticals, and travel support from Novartis, Roche, Bristol-Myers Squibb and Pierre Fabre Pharma, outside the submitted work. SH is on the advisory board or has received honoraria from Novartis, Pierre Fabre, BMS and MSD outside the submitted work. KD has received honoraria from Novartis, Pierre Fabre and Roche outside the submitted work. SF reports consulting or advisory board membership: Bayer, Illumina, Roche; honoraria: Amgen, Eli Lilly, PharmaMar, Roche; research funding: AstraZeneca, Pfizer, PharmaMar, Roche; travel or accommodation expenses: Amgen, Eli Lilly, Illumina, PharmaMar, Roche. JSU is on the advisory board or has received honoraria and travel support from Amgen, Bristol Myers Squibb, GSK, Immunocore, LeoPharma, Merck Sharp and Dohme, Novartis, Pierre Fabre, Roche, Sanofi outside the submitted work ME has received honoraria and travel expenses from Novartis and Immunocore. SHo received travel support for participation in congresses, (speaker) honoraria and research grants from Almirall, UCB, Janssen, Novartis, LEO Pharma and Lilly outside of the present publication. SP has received travel support for participation in congresses and/or speaker honoraria from Abbvie, Lilly, MSD, Novartis, Pfizer and Sanofi outside of the present publication. SPo is on the advisory board or has received honoraria from Galenicum Derma, ISDIN, Cantabria Labs and Mesoestetic. RLB has received support from Castle Bioscience for the International Melanoma Pathology Study Group Symposium and Workshop. MG served as consultant to argenx (honoraria paid to institution) and Almirall and received honoraria for participation in advisory boards / travel support from Biotest, GSK, Janssen, Leo Pharma, Lilly, Novartis and UCB - all outside the scope of the submitted work. MVH received honoraria from MSD, BMS, Roche, Novartis, Sun Pharma, Sanofi, Almirall, Biofrontera, Galderma. The other authors declare no competing interests.
Figures


References
-
- Goodman, B. & Flaxman, S. European Union Regulations on Algorithmic Decision-Making and a “Right to Explanation”. AI Mag.38, 50–57 (2017).
-
- Tonekaboni, S., Joshi, S., McCradden, M. D. & Goldenberg, A. What Clinicians Want: Contextualizing Explainable Machine Learning for Clinical End Use. In Proceedings of the 4th Machine Learning for Healthcare Conference 359–380 (PMLR, 2019).
