

Long term management of people with post-tuberculosis lung disease
- PMID: 38225822
- PMCID: PMC10790047
- DOI: 10.3904/kjim.2023.395
Long term management of people with post-tuberculosis lung disease
Abstract
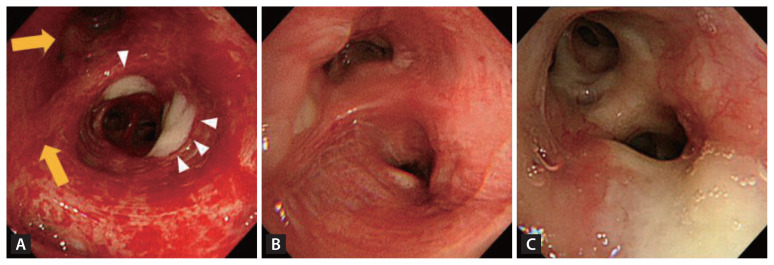
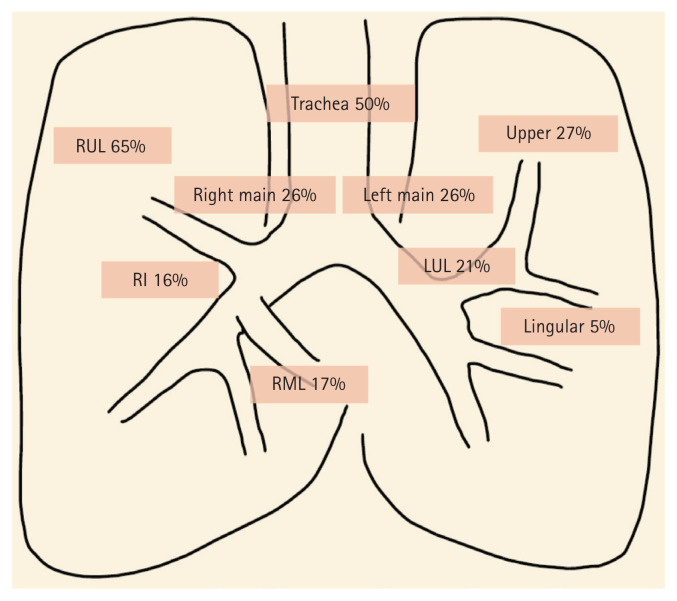
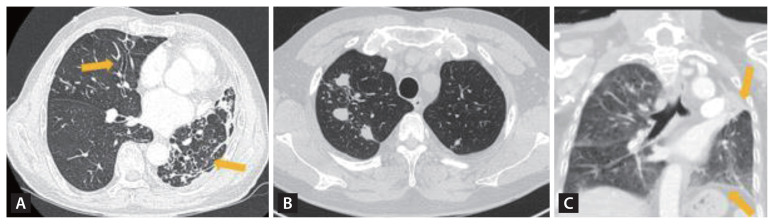
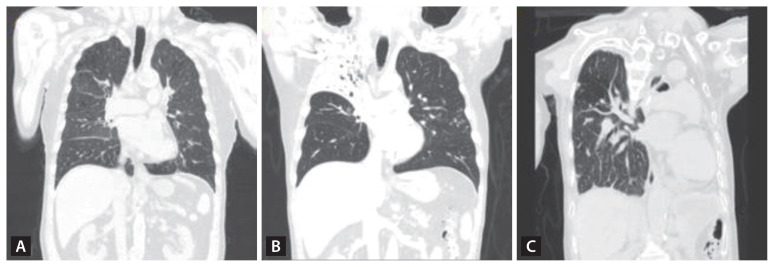
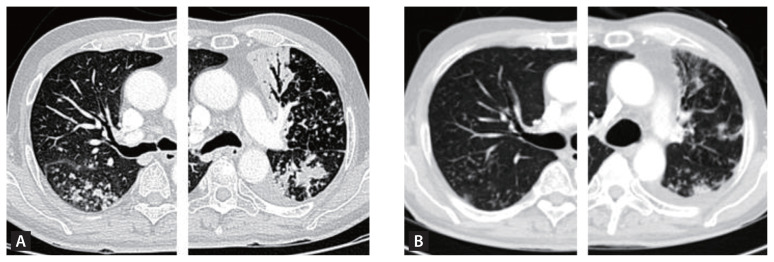
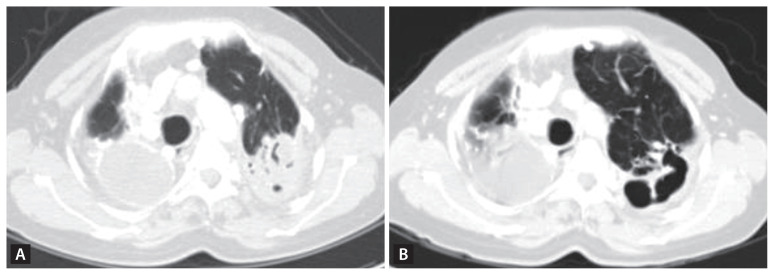
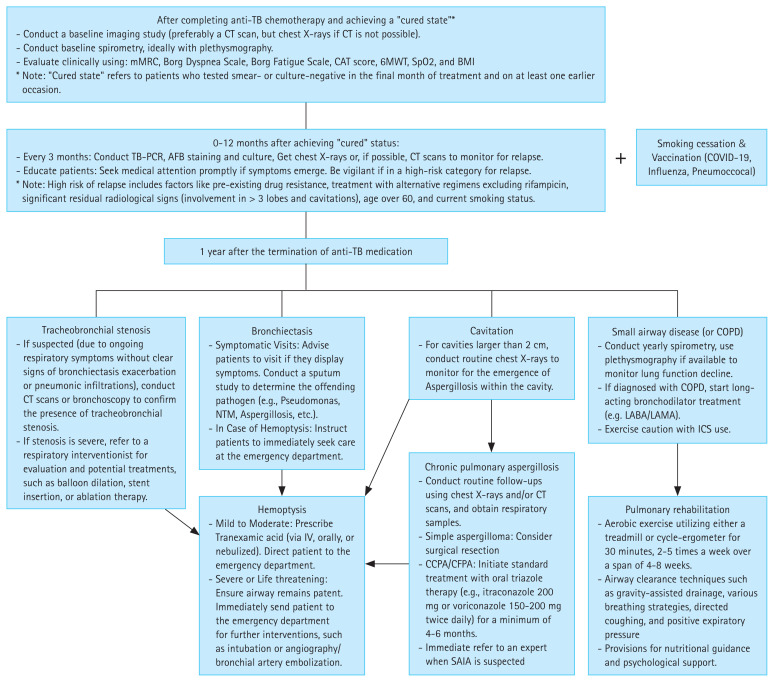
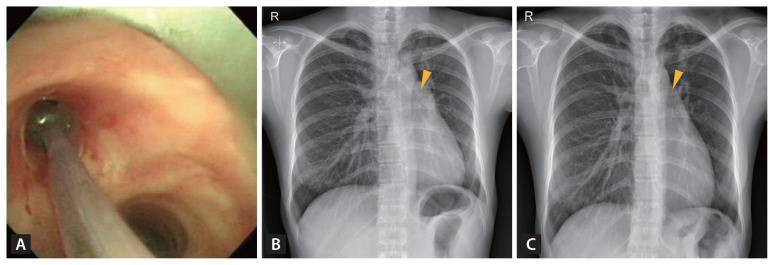
Post-tuberculosis lung disease (PTLD) is emerging as a significant area of global interest. As the number of patients surviving tuberculosis (TB) increases, the subsequent long-term repercussions have drawn increased attention due to their profound clinical and socioeconomic impacts. A primary obstacle to its comprehensive study has been its marked heterogeneity. The disease presents a spectrum of clinical manifestations which encompass tracheobronchial stenosis, bronchiectasis, granulomas with fibrosis, cavitation with associated aspergillosis, chronic pleural diseases, and small airway diseases-all persistent consequences of PTLD. The spectrum of symptoms a patient may experience varies based on the severity of the initial infection and the efficacy of the treatment received. As a result, the long-term management of PTLD necessitates a detailed and specific approach, addressing each manifestation individually-a tailored strategy. In the immediate aftermath (0-12 months after anti-TB chemotherapy), there should be an emphasis on monitoring for relapse, tracheobronchial stenosis, and smoking cessation. Subsequent management should focus on addressing hemoptysis, managing infection including aspergillosis, and TB-associated chronic obstructive pulmonary disease or restrictive lung function. There remains a vast expanse of knowledge to be discovered in PTLD. This review emphasizes the pressing need for comprehensive, consolidated guidelines for management of patients with PTLD.
Keywords: Aspergillosis; Bronchiectasis; Chronic obstructive pulmonary disease; Tuberculosis.
Conflict of interest statement
The authors disclose no conflicts.
Figures
Similar articles
-
Understanding the Spectrum and Management of Post-Tuberculosis Lung Disease: A Comprehensive Review.Cureus. 2024 Jun 28;16(6):e63420. doi: 10.7759/cureus.63420. eCollection 2024 Jun. Cureus. 2024. PMID: 39077302 Free PMC article. Review.
-
Post-Tuberculosis Lung Disease: Clinical Review of an Under-Recognised Global Challenge.Respiration. 2021;100(8):751-763. doi: 10.1159/000512531. Epub 2021 Jan 5. Respiration. 2021. PMID: 33401266 Review.
-
Chronic Pulmonary Aspergillosis as a Considerable Complication in Post-Tuberculosis Lung Disease.Semin Respir Crit Care Med. 2024 Feb;45(1):102-113. doi: 10.1055/s-0043-1776913. Epub 2024 Jan 9. Semin Respir Crit Care Med. 2024. PMID: 38196060 Review.
-
Implementation of spirometry screening for post-tuberculosis lung disease (PTLD) among adolescents and adults enrolled within the National Tuberculosis Control Program of Carmelo Hospital in Chókwè District, Mozambique: A hybrid type III effectiveness-implementation study protocol.BMC Pulm Med. 2024 Oct 10;24(1):502. doi: 10.1186/s12890-024-03329-7. BMC Pulm Med. 2024. PMID: 39390443 Free PMC article.
-
Post-tuberculosis lung disease in children and adolescents: A scoping review of definitions, measuring tools, and research gaps.Paediatr Respir Rev. 2025 Mar;53:55-63. doi: 10.1016/j.prrv.2024.07.001. Epub 2024 Jul 18. Paediatr Respir Rev. 2025. PMID: 39129097
Cited by
-
Is Pulmonary Mycoses Shadowed by Tuberculosis? Mandate to Hit the Bull's Eye-An Indian Perspective.Pathogens. 2025 Apr 30;14(5):435. doi: 10.3390/pathogens14050435. Pathogens. 2025. PMID: 40430764 Free PMC article. Review.
-
Understanding the Spectrum and Management of Post-Tuberculosis Lung Disease: A Comprehensive Review.Cureus. 2024 Jun 28;16(6):e63420. doi: 10.7759/cureus.63420. eCollection 2024 Jun. Cureus. 2024. PMID: 39077302 Free PMC article. Review.
-
Bridging science and policy in tuberculosis treatment through innovations in precision medicine, drug development, and cohort research: a narrative review.Ewha Med J. 2025 Apr;48(2):e22. doi: 10.12771/emj.2025.00115. Epub 2025 Apr 2. Ewha Med J. 2025. PMID: 40703366 Free PMC article. Review.
-
Comprehensive care for people affected by TB: addressing TB-associated disabilities.IJTLD Open. 2024 May 1;1(5):195-196. doi: 10.5588/ijtldopen.24.0167. eCollection 2024 May. IJTLD Open. 2024. PMID: 39022780 Free PMC article. No abstract available.
-
Assessment of comorbidities, risk factors, and post tuberculosis lung disease in National Tuberculosis Guidelines: A scoping review.PLOS Glob Public Health. 2025 Jul 23;5(7):e0004935. doi: 10.1371/journal.pgph.0004935. eCollection 2025. PLOS Glob Public Health. 2025. PMID: 40700421 Free PMC article.
References
-
- Wordl Health Organization . Global tuberculosis report 2022. Geneva: World Health Organization; 2022.
-
- Iseman MD. Tuberculosis therapy: past, present and future. Eur Respir J Suppl. 2002;36:87s–94s. - PubMed
-
- Snider GL. Tuberculosis then and now: a personal perspective on the last 50 years. Ann Intern Med. 1997;126:237–243. - PubMed
-
- Allwood B, van der Zalm M, Makanda G, Mortimer K, Steering Committee of the First International Post-Tuberculosis Symposium The long shadow post-tuberculosis. Lancet Infect Dis. 2019;19:1170–1171. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials