

Default Palliative Care Consultation for Seriously Ill Hospitalized Patients: A Pragmatic Cluster Randomized Trial
- PMID: 38227032
- PMCID: PMC10792472
- DOI: 10.1001/jama.2023.25092
Default Palliative Care Consultation for Seriously Ill Hospitalized Patients: A Pragmatic Cluster Randomized Trial
Abstract
Importance: Increasing inpatient palliative care delivery is prioritized, but large-scale, experimental evidence of its effectiveness is lacking.
Objective: To determine whether ordering palliative care consultation by default for seriously ill hospitalized patients without requiring greater palliative care staffing increased consultations and improved outcomes.
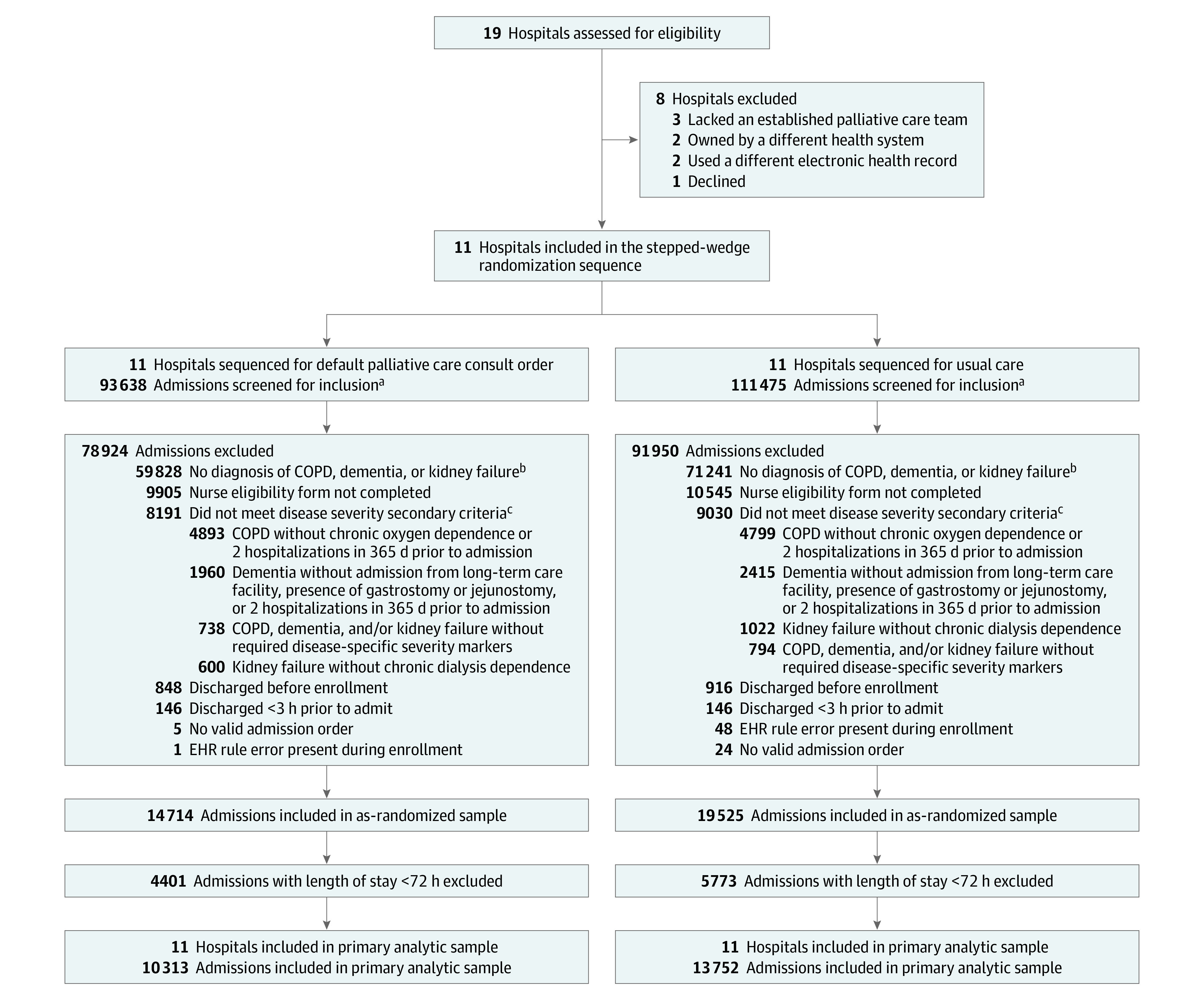
Design, setting, and participants: A pragmatic, stepped-wedge, cluster randomized trial was conducted among patients 65 years or older with advanced chronic obstructive pulmonary disease, dementia, or kidney failure admitted from March 21, 2016, through November 14, 2018, to 11 US hospitals. Outcome data collection ended on January 31, 2019.
Intervention: Ordering palliative care consultation by default for eligible patients, while allowing clinicians to opt-out, was compared with usual care, in which clinicians could choose to order palliative care.
Main outcomes and measures: The primary outcome was hospital length of stay, with deaths coded as the longest length of stay, and secondary end points included palliative care consult rate, discharge to hospice, do-not-resuscitate orders, and in-hospital mortality.
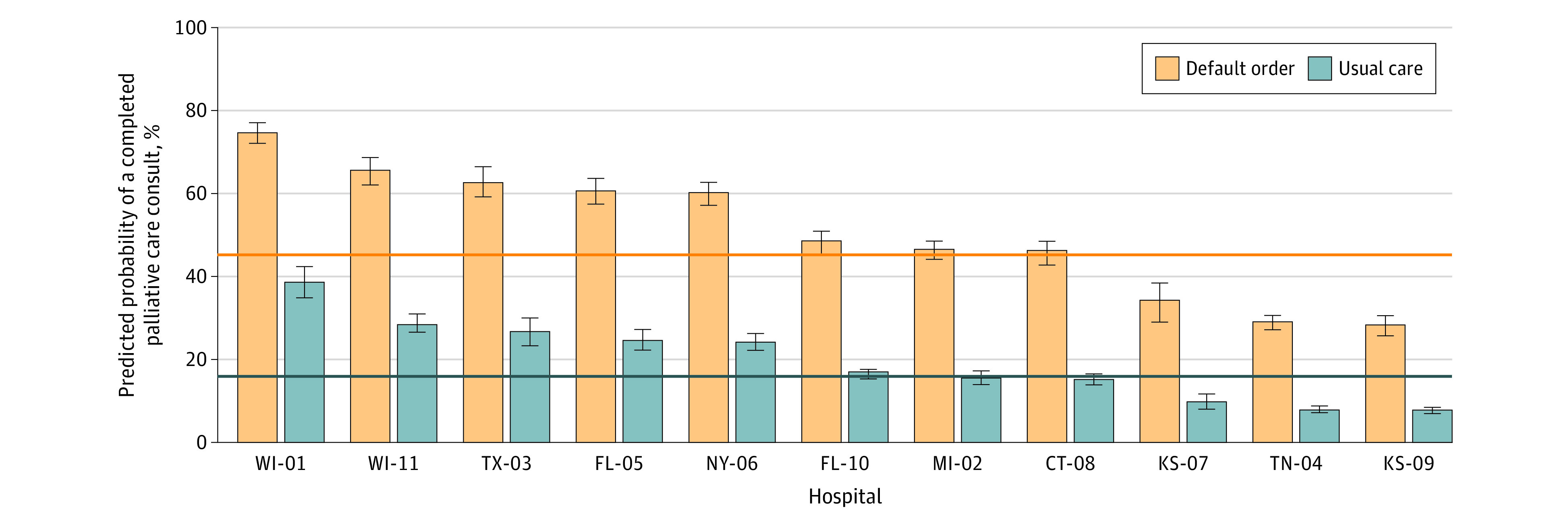
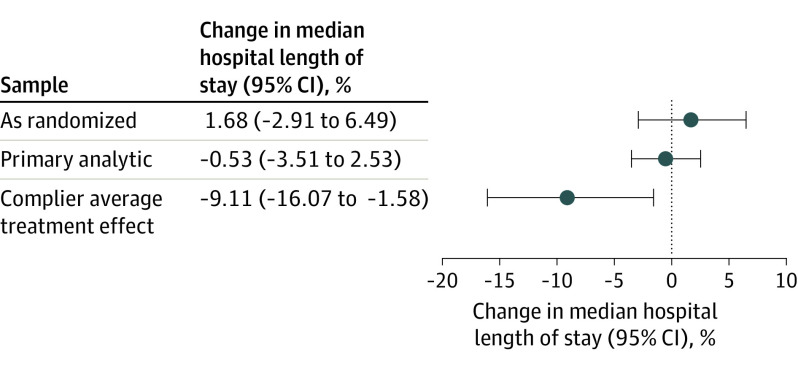
Results: Of 34 239 patients enrolled, 24 065 had lengths of stay of at least 72 hours and were included in the primary analytic sample (10 313 in the default order group and 13 752 in the usual care group; 13 338 [55.4%] women; mean age, 77.9 years). A higher percentage of patients in the default order group received palliative care consultation than in the standard care group (43.9% vs 16.6%; adjusted odds ratio [aOR], 5.17 [95% CI, 4.59-5.81]) and received consultation earlier (mean [SD] of 3.4 [2.6] days after admission vs 4.6 [4.8] days; P < .001). Length of stay did not differ between the default order and usual care groups (percent difference in median length of stay, -0.53% [95% CI, -3.51% to 2.53%]). Patients in the default order group had higher rates of do-not-resuscitate orders at discharge (aOR, 1.40 [95% CI, 1.21-1.63]) and discharge to hospice (aOR, 1.30 [95% CI, 1.07-1.57]) than the usual care group, and similar in-hospital mortality (4.7% vs 4.2%; aOR, 0.86 [95% CI, 0.68-1.08]).
Conclusions and relevance: Default palliative care consult orders did not reduce length of stay for older, hospitalized patients with advanced chronic illnesses, but did improve the rate and timing of consultation and some end-of-life care processes.
Trial registration: ClinicalTrials.gov Identifier: NCT02505035.
Conflict of interest statement
Figures
Comment in
-
A Tale of 2 Palliative Care Trials: Developing Sustainable and Transferable Models.JAMA. 2024 Jan 16;331(3):196-198. doi: 10.1001/jama.2023.26815. JAMA. 2024. PMID: 38227043 Free PMC article. No abstract available.
References
-
- A National Framework and Preferred Practices for Palliative and Hospice Care Quality. National Quality Forum ; 2006.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
