

Nurse and Social Worker Palliative Telecare Team and Quality of Life in Patients With COPD, Heart Failure, or Interstitial Lung Disease: The ADAPT Randomized Clinical Trial
- PMID: 38227034
- PMCID: PMC10792473
- DOI: 10.1001/jama.2023.24035
Nurse and Social Worker Palliative Telecare Team and Quality of Life in Patients With COPD, Heart Failure, or Interstitial Lung Disease: The ADAPT Randomized Clinical Trial
Erratum in
-
Corrected Data Presentation.JAMA. 2025 Apr 15;333(15):1364. doi: 10.1001/jama.2025.3767. JAMA. 2025. PMID: 40136260 Free PMC article. No abstract available.
Abstract
Importance: Many patients with chronic obstructive pulmonary disease (COPD), heart failure (HF), and interstitial lung disease (ILD) endure poor quality of life despite conventional therapy. Palliative care approaches may benefit this population prior to end of life.
Objective: Determine the effect of a nurse and social worker palliative telecare team on quality of life in outpatients with COPD, HF, or ILD compared with usual care.
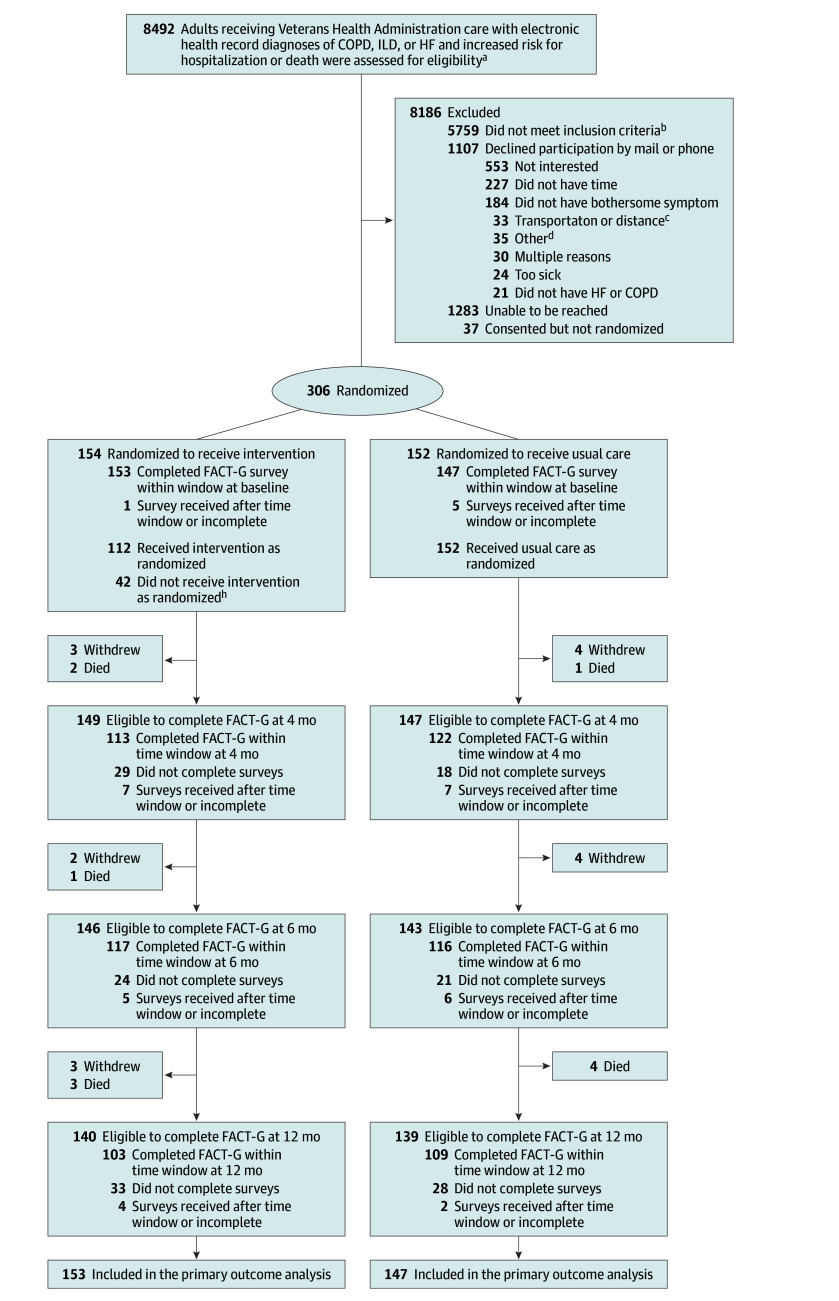
Design, setting, and participants: Single-blind, 2-group, multisite randomized clinical trial with accrual between October 27, 2016, and April 2, 2020, in 2 Veterans Administration health care systems (Colorado and Washington), and including community-based outpatient clinics. Outpatients with COPD, HF, or ILD at high risk of hospitalization or death who reported poor quality of life participated.
Intervention: The intervention involved 6 phone calls with a nurse to help with symptom management and 6 phone calls with a social worker to provide psychosocial care. The nurse and social worker met weekly with a study primary care and palliative care physician and as needed, a pulmonologist, and cardiologist. Usual care included an educational handout developed for the study that outlined self-care for COPD, ILD, or HF. Patients in both groups received care at the discretion of their clinicians, which could include care from nurses and social workers, and specialists in cardiology, pulmonology, palliative care, and mental health.
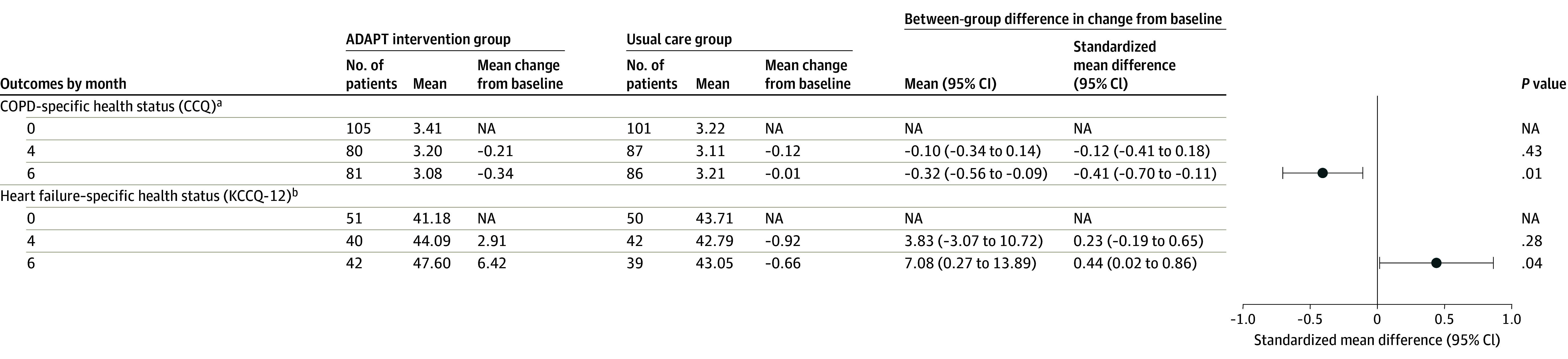
Main outcomes and measures: The primary outcome was difference in change in quality of life from baseline to 6 months between the intervention and usual care groups (FACT-G score range, 0-100, with higher scores indicating better quality of life, clinically meaningful change ≥4 points). Secondary quality-of-life outcomes at 6 months included disease-specific health status (Clinical COPD Questionnaire; Kansas City Cardiomyopathy Questionnaire-12), depression (Patient Health Questionnaire-8) and anxiety (Generalized Anxiety Disorder-7) symptoms.
Results: Among 306 randomized patients (mean [SD] age, 68.9 [7.7] years; 276 male [90.2%], 30 female [9.8%]; 245 White [80.1%]), 177 (57.8%) had COPD, 67 (21.9%) HF, 49 (16%) both COPD and HF, and 13 (4.2%) ILD. Baseline FACT-G scores were similar (intervention, 52.9; usual care, 52.7). FACT-G completion was 76% (intervention, 117 of 154; usual care, 116 of 152) at 6 months for both groups. Mean (SD) length of intervention was 115.1 (33.4) days and included a mean of 10.4 (3.3) intervention calls per patient. In the intervention group, 112 of 154 (73%) patients received the intervention as randomized. At 6 months, mean FACT-G score improved 6.0 points in the intervention group and 1.4 points in the usual care group (difference, 4.6 points [95% CI, 1.8-7.4]; P = .001; standardized mean difference, 0.41). The intervention also improved COPD health status (standardized mean difference, 0.44; P = .04), HF health status (standardized mean difference, 0.41; P = .01), depression (standardized mean difference, -0.50; P < .001), and anxiety (standardized mean difference, -0.51; P < .001) at 6 months.
Conclusions and relevance: For adults with COPD, HF, or ILD who were at high risk of death and had poor quality of life, a nurse and social worker palliative telecare team produced clinically meaningful improvements in quality of life at 6 months compared with usual care.
Trial registration: ClinicalTrials.gov Identifier: NCT02713347.
Conflict of interest statement
Figures


Comment in
-
A Tale of 2 Palliative Care Trials: Developing Sustainable and Transferable Models.JAMA. 2024 Jan 16;331(3):196-198. doi: 10.1001/jama.2023.26815. JAMA. 2024. PMID: 38227043 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
