

Association of Mild Iodine Insufficiency during Pregnancy with Child Neurodevelopment in Patients with Subclinical Hypothyroidism or Hypothyroxinemia
- PMID: 38228158
- PMCID: PMC11153033
- DOI: 10.1055/s-0043-1778037
Association of Mild Iodine Insufficiency during Pregnancy with Child Neurodevelopment in Patients with Subclinical Hypothyroidism or Hypothyroxinemia
Abstract
Objective: Our objective was to evaluate whether iodine status in pregnant patients with either subclinical hypothyroidism or hypothyroxinemia in the first half of pregnancy is associated with measures of behavior and neurodevelopment in children through the age of 5 years.
Study design: This is a secondary analysis of a multicenter study consisting of two randomized, double-masked, placebo-controlled treatment trials conducted in parallel. Patients with a singleton gestation before 20 weeks' gestation underwent thyroid screening using serum thyrotropin and free thyroxine. Participants with subclinical hypothyroidism or hypothyroxinemia were randomized to levothyroxine replacement or an identical placebo. At randomization, maternal urine was collected and stored for subsequent urinary iodine excretion analysis. Urinary iodine concentrations greater than 150 μg/L were considered iodine sufficient, and concentrations of 150 μg/L or less were considered iodine insufficient. The primary outcome was a full-scale intelligence quotient (IQ) score at the age of 5 years, the general conceptual ability score from the Differential Ability Scales-II at the age of 3 if IQ was not available, or death before 3 years.
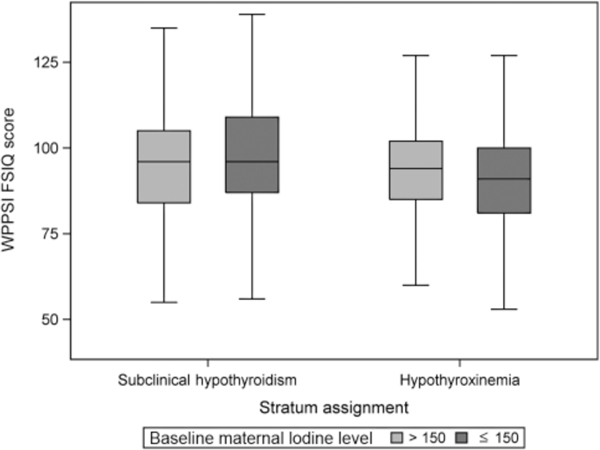
Results: A total of 677 pregnant participants with subclinical hypothyroidism and 526 with hypothyroxinemia were randomized. The primary outcome was available in 1,133 (94%) of children. Overall, 684 (60%) of mothers were found to have urinary iodine concentrations >150 μg/L. Children of iodine-sufficient participants with subclinical hypothyroidism had similar primary outcome scores when compared to children of iodine-insufficient participants (95 [84-105] vs. 96 [87-109], P adj = 0.73). After adjustment, there was also no difference in IQ scores among children of participants with hypothyroxinemia at 5 to 7 years of age (94 [85 - 102] and 91 [81 - 100], Padj 1/4 0.11). Treatment with levothyroxine was not associated with neurodevelopmental or behavioral outcomes regardless of maternal iodine status (p > 0.05).
Conclusion: Maternal urinary iodine concentrations ≤150 μg/L were not associated with abnormal cognitive or behavioral outcomes in offspring of participants with either subclinical hypothyroidism or hypothyroxinemia.
Key points: · Most pregnant patients with subclinical thyroid disease are iodine sufficient.. · Mild maternal iodine insufficiency is not associated with lower offspring IQ at 5 years.. · Iodine supplementation in subclinical thyroid disease is unlikely to improve IQ..
Thieme. All rights reserved.
Conflict of interest statement
None declared.
Figures
References
-
- De Leo S, Pearce EN, Braverman LE. Iodine supplementation in women during preconception, pregnancy, and lactation: current clinical practice by U.S. obstetricians and midwives. Thyroid 2017;27(03):434–439 - PubMed
-
- Haddow JE, Palomaki GE, Allan WC, et al. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med 1999;341(08):549–555 - PubMed
-
- Pop VJ, Kuijpens JL, van Baar AL, et al. Low maternal free thyroxine concentrations during early pregnancy are associated with impaired psychomotor development in infancy. Clin Endocrinol (oxf) 1999;50(02):149–155 - PubMed
-
- Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, de Vijlder JJ. Maternal hypothyroxinaemia during early pregnancy and subsequent child development: a 3-year follow-up study. Clin Endocrinol (Oxf) 2003;59(03):282–288 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 HD053118/HD/NICHD NIH HHS/United States
- U10 HD040500/HD/NICHD NIH HHS/United States
- UG1 HD027869/HD/NICHD NIH HHS/United States
- U10 HD040544/HD/NICHD NIH HHS/United States
- UG1 HD034116/HD/NICHD NIH HHS/United States
- UG1 HD040560/HD/NICHD NIH HHS/United States
- UG1 HD087230/HD/NICHD NIH HHS/United States
- UG1 HD053097/HD/NICHD NIH HHS/United States
- U10 HD040485/HD/NICHD NIH HHS/United States
- U10 HD034116/HD/NICHD NIH HHS/United States
- U10 HD027869/HD/NICHD NIH HHS/United States
- U10 HD027917/HD/NICHD NIH HHS/United States
- UG1 HD040485/HD/NICHD NIH HHS/United States
- U10 HD040560/HD/NICHD NIH HHS/United States
- UG1 HD040500/HD/NICHD NIH HHS/United States
- U10 HD040512/HD/NICHD NIH HHS/United States
- U10 HD040545/HD/NICHD NIH HHS/United States
- U01 HD036801/HD/NICHD NIH HHS/United States
- UG1 HD027915/HD/NICHD NIH HHS/United States
- UG1 HD087192/HD/NICHD NIH HHS/United States
- UG1 HD040544/HD/NICHD NIH HHS/United States
- UG1 HD034208/HD/NICHD NIH HHS/United States
- UG1 HD040512/HD/NICHD NIH HHS/United States
- U10 HD027915/HD/NICHD NIH HHS/United States
- UG1 HD040545/HD/NICHD NIH HHS/United States
- U10 HD034208/HD/NICHD NIH HHS/United States
- U10 HD053097/HD/NICHD NIH HHS/United States
- U10 HD021410/HD/NICHD NIH HHS/United States
- U10 HD036801/HD/NICHD NIH HHS/United States
- U24 HD036801/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
