

HHV-6B detection and host gene expression implicate HHV-6B as pulmonary pathogen after hematopoietic cell transplant
- PMID: 38228644
- PMCID: PMC10791683
- DOI: 10.1038/s41467-024-44828-9
HHV-6B detection and host gene expression implicate HHV-6B as pulmonary pathogen after hematopoietic cell transplant
Abstract
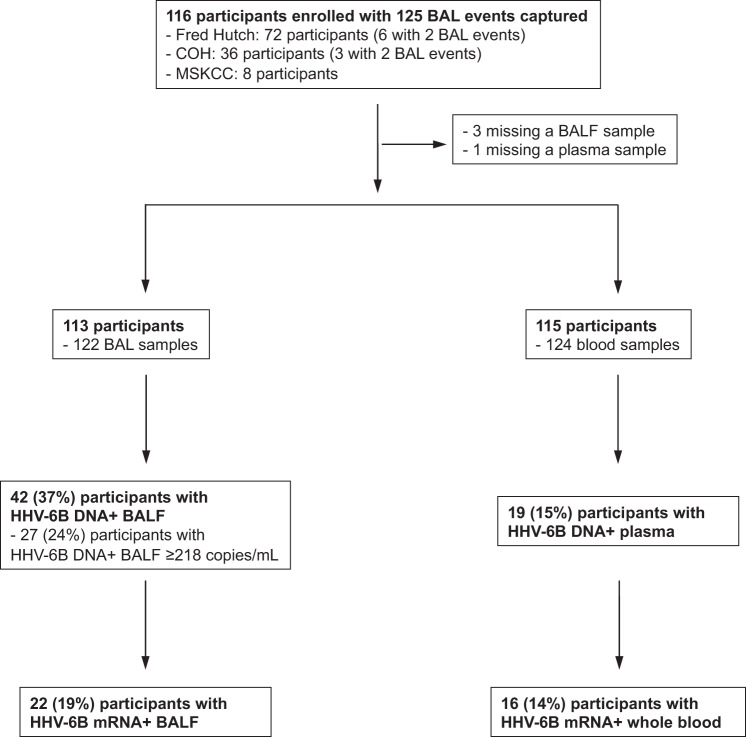
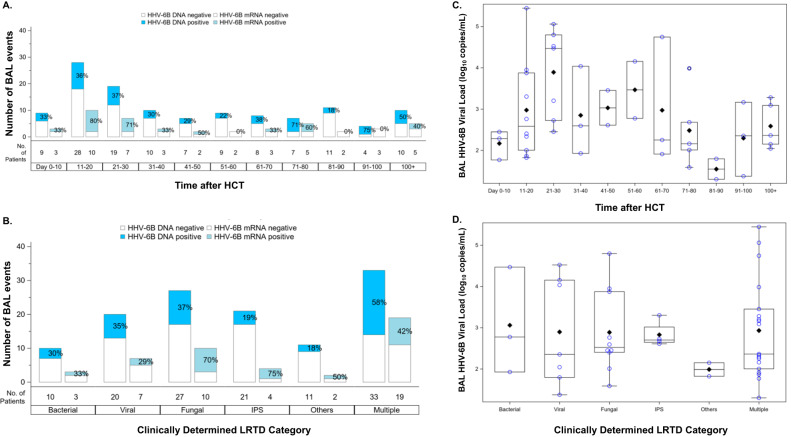
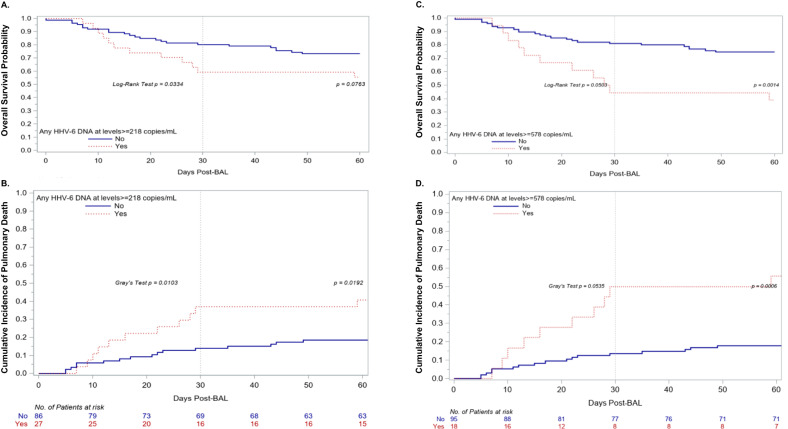
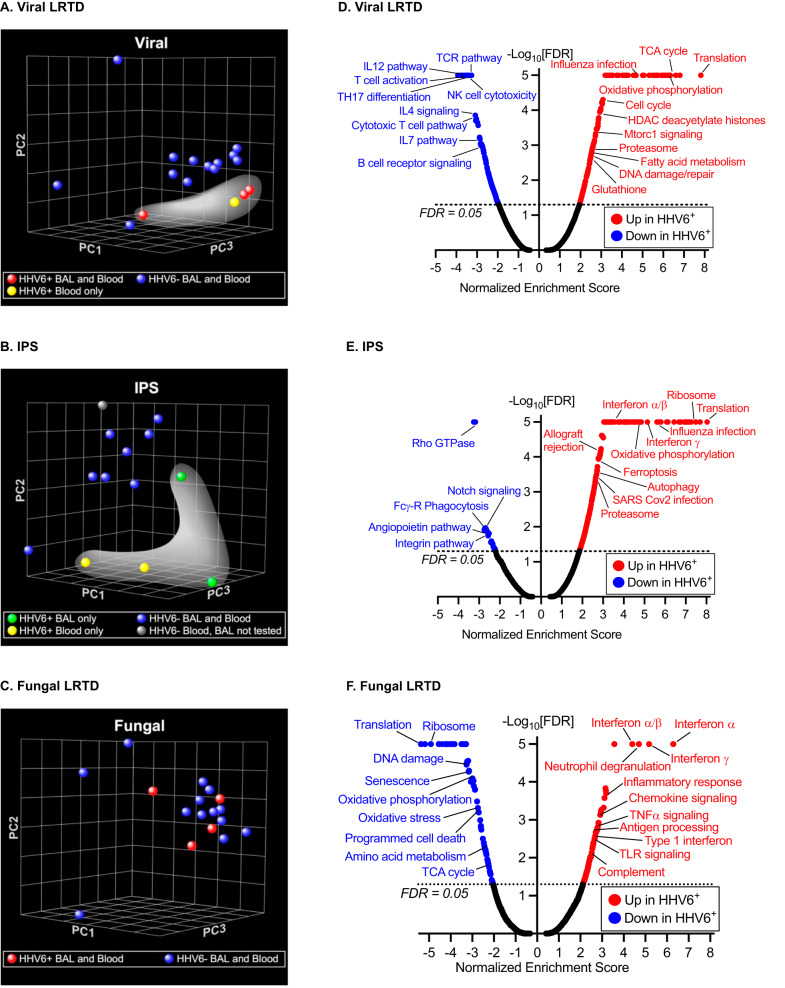
Limited understanding of the immunopathogenesis of human herpesvirus 6B (HHV-6B) has prevented its acceptance as a pulmonary pathogen after hematopoietic cell transplant (HCT). In this prospective multicenter study of patients undergoing bronchoalveolar lavage (BAL) for pneumonia after allogeneic HCT, we test blood and BAL fluid (BALF) for HHV-6B DNA and mRNA transcripts associated with lytic infection and perform RNA-seq on paired blood. Among 116 participants, HHV-6B DNA is detected in 37% of BALs, 49% of which also have HHV-6B mRNA detection. We establish HHV-6B DNA viral load thresholds in BALF that are highly predictive of HHV-6B mRNA detection and associated with increased risk for overall mortality and death from respiratory failure. Participants with HHV-6B DNA in BALF exhibit distinct host gene expression signatures, notable for enriched interferon signaling pathways in participants clinically diagnosed with idiopathic pneumonia. These data implicate HHV-6B as a pulmonary pathogen after allogeneic HCT.
© 2024. The Author(s).
Conflict of interest statement
The authors declare the following financial competing interests. J.A.H.: Consulting for Allovir, Gilead, Karius, Symbio; research support from Allovir, Gilead, Karius, Merck. Y.J.L.: Research support from Karius, AiCuris, Scynexis, and Merck & Co Inc. A.W.: Consulting for Kyorin Pharmaceutical and Vir; research support from Allovir, Ansun Biopharma, Pfizer, Vir/GSK. G.R.H.: Consulting for Generon Corporation, NapaJen Pharma, iTeos Therapeutics, Neoleukin Therapeutics, Commonwealth Serum Laboratories, Cynata Therapeutics; research support from Compass Therapeutics, Syndax Pharmaceuticals, Applied Molecular Transport, Serplus Technology, Heat Biologics, Laevoroc Oncology, iTEOS therapetics and Genentech. D.M.Z.: Consulting for Allovir. S.S.D.: Consulting for Allovir, Asepticope, Merck, Takeda, Astellas Pharma; research support from Allovir, Ansun Biopharma, Karius, Merck. M.B.: Consulting for Allovir, Symbio, Evrys Bio; research support from Merck. L.K.V., H.X., E.L.C., G.S.C., H.Z., M.L.H., K.R.J., W.L., S.G. and S.J. declare no financial competing interests. All authors have no non-financial interests to declare.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
