

Pharmacist-led intervention for older people with atrial fibrillation in long-term care (PIVOTALL study): a randomised pilot and feasibility study
- PMID: 38229013
- PMCID: PMC10790530
- DOI: 10.1186/s12877-023-04527-4
Pharmacist-led intervention for older people with atrial fibrillation in long-term care (PIVOTALL study): a randomised pilot and feasibility study
Abstract
Background: Older care home residents are a vulnerable group of people with atrial fibrillation (AF) at high risk of adverse health events. The Atrial Fibrillation Better Care (ABC: Avoid stroke; Better symptom management; Cardiovascular and other comorbidity management) pathway is the gold-standard approach toward integrated AF care, and pharmacists are a potential resource with regards to its' implementation. The aim of this study was to determine the feasibility of pharmacist-led medicines optimisation in care home residents, based on the ABC pathway compared to usual care.
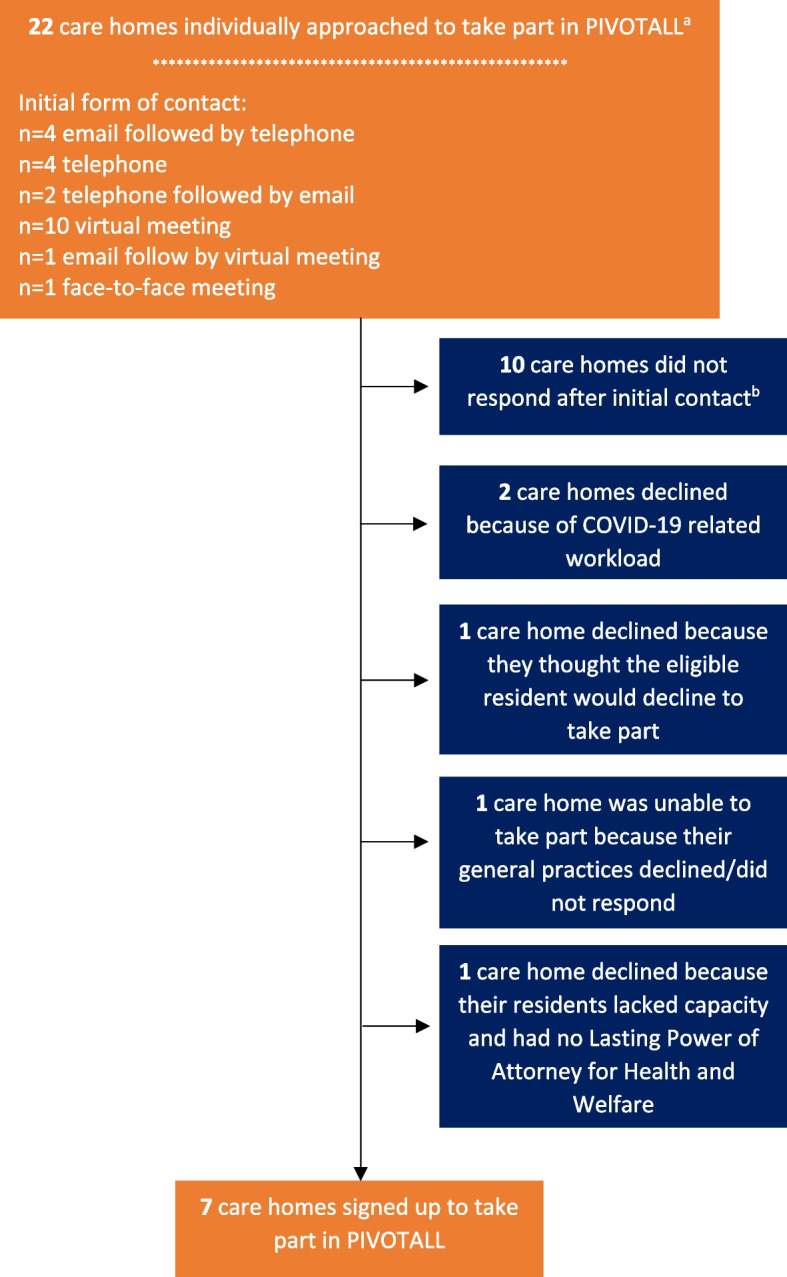
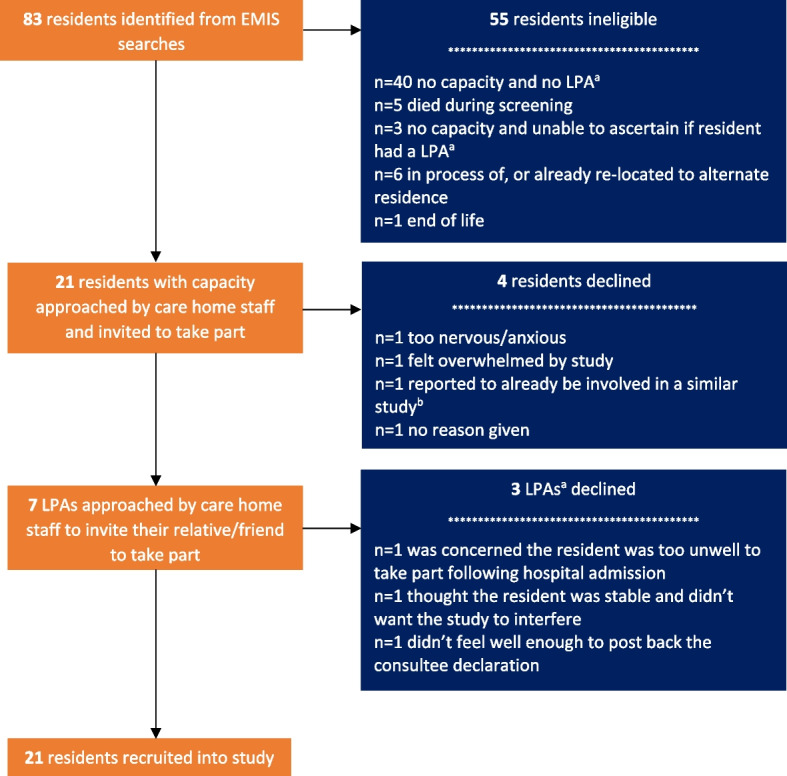
Methods: Individually randomised, prospective pilot and feasibility study of older (aged ≥ 65 years) care home residents with AF (ISRCTN14747952); residents randomised to ABC pathway optimised care versus usual care. The primary outcome was a description of study feasibility (resident and care home recruitment and retention). Secondary outcomes included the number and type of pharmacist medication recommendations and general practitioner (GP) implementation.
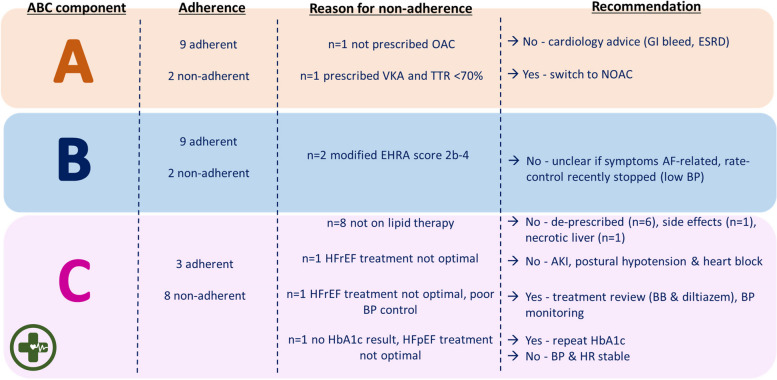
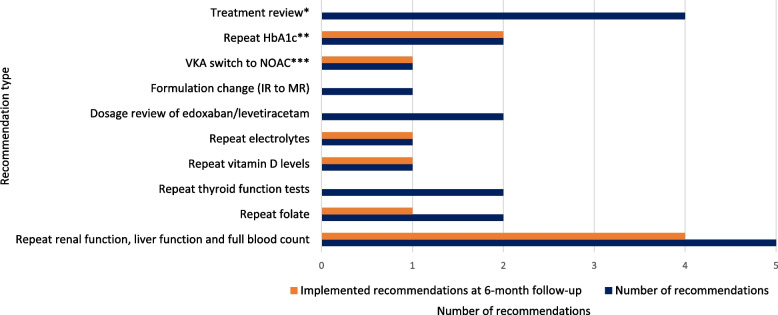
Results: Twenty-one residents were recruited and 11 (mean age [standard deviation] 85.0 [6.5] years, 63.6% female) were randomised to receive pharmacist-led medicines optimisation. Only 3/11 residents were adherent to all three components of the ABC pathway. Adherence was higher to 'A' (9/11 residents) and 'B' (9/11 residents) components compared to 'C' (3/11 residents). Four ABC-specific medicines recommendations were made for three residents, and two were implemented by residents' GPs. Overall ABC adherence rates did not change after pharmacist medication review, but adherence to 'A' increased (from 9/11 to 10/11 residents). Other ABC recommendations were inappropriate given residents' co-morbidities and risk of medication-related adverse effects.
Conclusions: The ABC pathway as a framework was feasible to implement for pharmacist medication review, but most residents' medications were already optimised. Low rates of adherence to guideline-recommended therapy were a result of active decisions not to treat after assessment of the net risk-benefit.
Keywords: Atrial fibrillation; Care homes; Feasibility study; Integrated care; Medication optimisation; Older people; Pharmacists.
© 2024. The Author(s).
Conflict of interest statement
PEP owns four shares in AstraZeneca PLC and has received honoraria and/or travel reimbursement for events sponsored by AKCEA, Amgen, AMRYT, Link Medical, Napp, Sanofi. GYHL has been a consultant and speaker for BMS/Pfizer, Boehringer Ingelheim, Anthos and Daiichi-Sankyo, no fees are received personally. GYHL is co-principal investigator of the AFFIRMO project on multimorbidity in AF, which has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 899871. DAL has received investigator-initiated educational grants from Bristol-Myers Squibb (BMS), has been a speaker for Bayer, Boehringer Ingelheim, and BMS/Pfizer and has consulted for BMS, and Boehringer Ingelheim; LAR and AA have no competing interests to report.
Figures
Similar articles
-
Adherence to the Atrial fibrillation Better Care pathway and the risk of adverse health outcomes in older care home residents with atrial fibrillation: a retrospective data linkage study 2003-18.Age Ageing. 2024 Feb 1;53(2):afae021. doi: 10.1093/ageing/afae021. Age Ageing. 2024. PMID: 38400634 Free PMC article.
-
Protocol for a cluster randomised controlled trial to determine the effectiveness and cost-effectiveness of independent pharmacist prescribing in care homes: the CHIPPS study.Trials. 2020 Jan 21;21(1):103. doi: 10.1186/s13063-019-3827-0. Trials. 2020. PMID: 31964398 Free PMC article.
-
Residential medication management reviews of antithrombotic therapy in aged care residents with atrial fibrillation: assessment of stroke and bleeding risk.J Clin Pharm Ther. 2016 Jun;41(3):279-84. doi: 10.1111/jcpt.12385. Epub 2016 Apr 7. J Clin Pharm Ther. 2016. PMID: 27062272
-
The Atrial Fibrillation Better Care pathway for managing atrial fibrillation: a review.Europace. 2021 Oct 9;23(10):1511-1527. doi: 10.1093/europace/euab092. Europace. 2021. PMID: 34125202 Free PMC article. Review.
-
Integrated Care for Atrial Fibrillation Management: The Role of the Pharmacist.Am J Med. 2022 Dec;135(12):1410-1426. doi: 10.1016/j.amjmed.2022.07.014. Epub 2022 Aug 21. Am J Med. 2022. PMID: 36002045 Review.
Cited by
-
Service delivery and the role of clinical pharmacists in UK primary care for older people, including people with dementia: a scoping review.BMC Prim Care. 2025 Jan 14;26(1):10. doi: 10.1186/s12875-024-02685-x. BMC Prim Care. 2025. PMID: 39810119 Free PMC article.
-
Quality of prescribing and health-related quality of life in older adults: a narrative review with a special focus on patients with atrial fibrillation and multimorbidity.Eur Geriatr Med. 2025 Mar 9. doi: 10.1007/s41999-025-01175-2. Online ahead of print. Eur Geriatr Med. 2025. PMID: 40059107 Review.
References
-
- World Health Organization. European Health Information Gateway. Number of nursing and elderly home beds. Available from: https://gateway.euro.who.int/en/indicators/hfa_491-5101-number-of-nursin... [cited 1 Jan 2023].
-
- World Health Organization. Partnering with the EU to strengthen long-term care systems. Available from: https://www.who.int/europe/activities/partnering-with-the-eu-to-strength... [cited 13 Nov 2023].
-
- Office for National Statistics. Care homes and estimating the self-funding population, England: 2021 to 2022. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/... [cited 08 Sept 2022].
-
- Benjamin Emelia J, Muntner P, Alonso A, BittencourtMarcio S, Callaway Clifton W, Carson April P, et al. Heart disease and stroke statistics—2019 Update: a report from the American Heart Association. Circulation. 2019;139(10):e56–e528. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
