

Clinical manifestations and EEG findings in children infected with COVID-19 and exhibiting neurological symptoms
- PMID: 38229077
- PMCID: PMC10790490
- DOI: 10.1186/s12887-023-04496-y
Clinical manifestations and EEG findings in children infected with COVID-19 and exhibiting neurological symptoms
Abstract
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV2) infection has many neurological manifestations, and its effects on the nervous system are increasingly recognized. There has been no systematic analysis of electroencephalography (EEG) characteristics in children exhibiting neurological symptoms of Coronavirus disease 2019 (COVID-19). The primary aim of this study was to describe the EEG characteristics caused by COVID-19 infection in children who were showing neurological symptoms and to assess the relationship between COVID-19-related EEG changes and clinical features in these children.
Method: This study included 125 pediatric patients infected with SARS-CoV2 and showing neurological symptoms, and their continuous EEG was recorded. In addition, the demographic and clinical characteristics of these patients were analyzed and the correlation between the two was investigated.
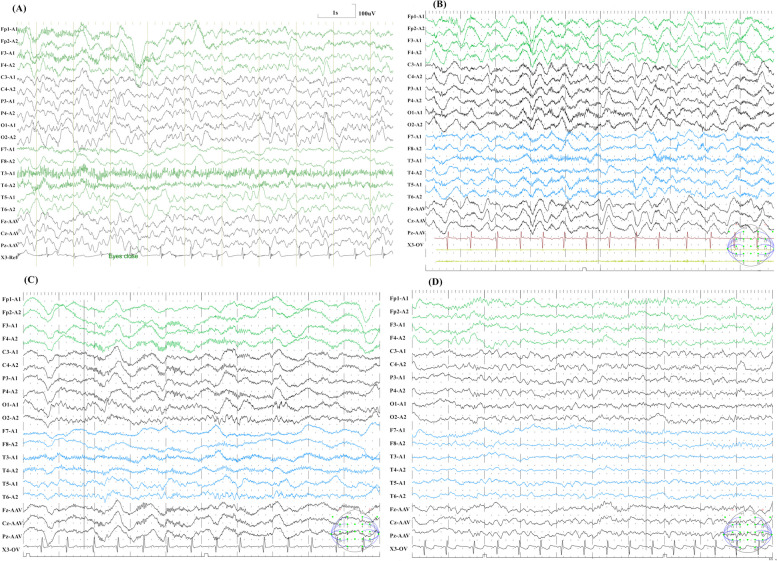
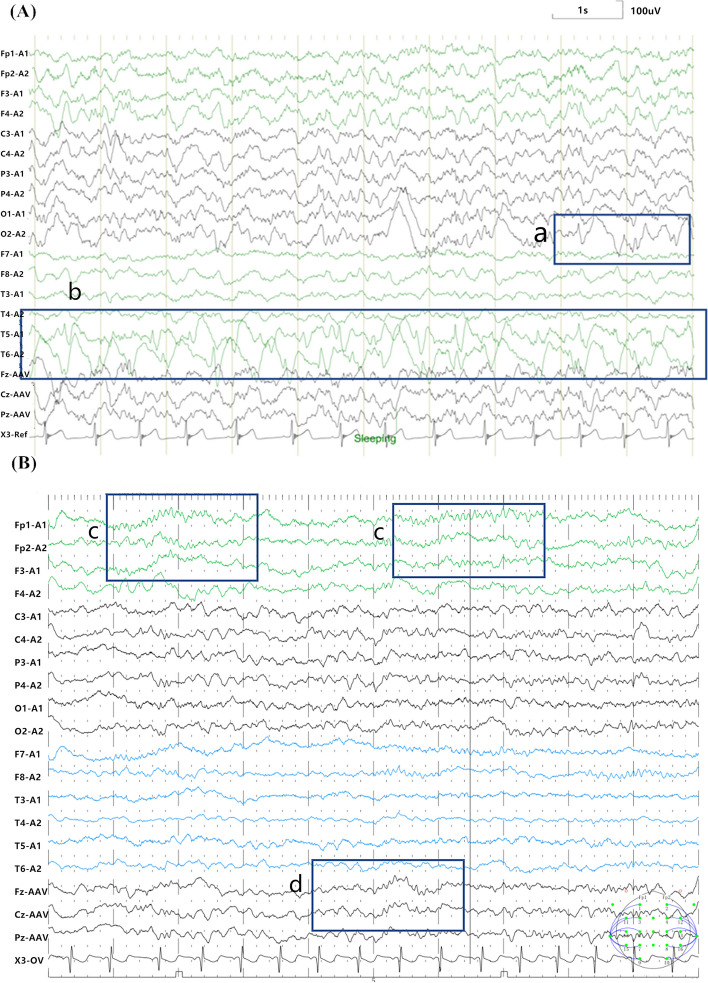
Results: Abnormal EEG findings were detected in 31.20% (N = 39) of the patients. Abnormal discharges (43.59%) were the most common EEG abnormalities, followed by background abnormalities (41.03%). The proportion of patients diagnosed with febrile seizure was higher in the normal EEG group than in the abnormal EEG group (P = 0.002), while the opposite was true for epilepsy and encephalitis/encephalopathy (P = 0.016 and P = 0.003, respectively). The independent associated factors of abnormal EEG were age and total length of stay (P < 0.001 and P = 0.003, respectively). Non-specific EEG abnormalities were found in COVID-19-related encephalitis/encephalopathy.
Conclusion: Our study corroborated that a small group of pediatric patients infected by COVID-19 and showing neurological symptoms may exhibit abnormal EEG. This study could help improve the understanding of clinical and EEG characteristics in children with COVID-19 and inform triage policies in other hospitals during the COVID-19 pandemic.
Keywords: COVID-19; EEG; Pediatrics; Seizures.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Physical interventions to interrupt or reduce the spread of respiratory viruses.Cochrane Database Syst Rev. 2023 Jan 30;1(1):CD006207. doi: 10.1002/14651858.CD006207.pub6. Cochrane Database Syst Rev. 2023. PMID: 36715243 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Antibody tests for identification of current and past infection with SARS-CoV-2.Cochrane Database Syst Rev. 2022 Nov 17;11(11):CD013652. doi: 10.1002/14651858.CD013652.pub2. Cochrane Database Syst Rev. 2022. PMID: 36394900 Free PMC article.
-
Measures implemented in the school setting to contain the COVID-19 pandemic.Cochrane Database Syst Rev. 2022 Jan 17;1(1):CD015029. doi: 10.1002/14651858.CD015029. Cochrane Database Syst Rev. 2022. Update in: Cochrane Database Syst Rev. 2024 May 2;5:CD015029. doi: 10.1002/14651858.CD015029.pub2. PMID: 35037252 Free PMC article. Updated.
-
Rapid, point-of-care antigen tests for diagnosis of SARS-CoV-2 infection.Cochrane Database Syst Rev. 2022 Jul 22;7(7):CD013705. doi: 10.1002/14651858.CD013705.pub3. Cochrane Database Syst Rev. 2022. PMID: 35866452 Free PMC article.
Cited by
-
Comparing clinical and biochemical characteristics of febrile seizures in children with and without COVID-19: a retrospective study.BMC Infect Dis. 2024 Dec 5;24(1):1389. doi: 10.1186/s12879-024-10287-2. BMC Infect Dis. 2024. PMID: 39639218 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
