

Symptom-based stratification of patients with primary Sjögren's syndrome: multi-dimensional characterisation of international observational cohorts and reanalyses of randomised clinical trials
- PMID: 38229348
- PMCID: PMC7134527
- DOI: 10.1016/S2665-9913(19)30042-6
Symptom-based stratification of patients with primary Sjögren's syndrome: multi-dimensional characterisation of international observational cohorts and reanalyses of randomised clinical trials
Abstract
Background: Heterogeneity is a major obstacle to developing effective treatments for patients with primary Sjögren's syndrome. We aimed to develop a robust method for stratification, exploiting heterogeneity in patient-reported symptoms, and to relate these differences to pathobiology and therapeutic response.
Methods: We did hierarchical cluster analysis using five common symptoms associated with primary Sjögren's syndrome (pain, fatigue, dryness, anxiety, and depression), followed by multinomial logistic regression to identify subgroups in the UK Primary Sjögren's Syndrome Registry (UKPSSR). We assessed clinical and biological differences between these subgroups, including transcriptional differences in peripheral blood. Patients from two independent validation cohorts in Norway and France were used to confirm patient stratification. Data from two phase 3 clinical trials were similarly stratified to assess the differences between subgroups in treatment response to hydroxychloroquine and rituximab.
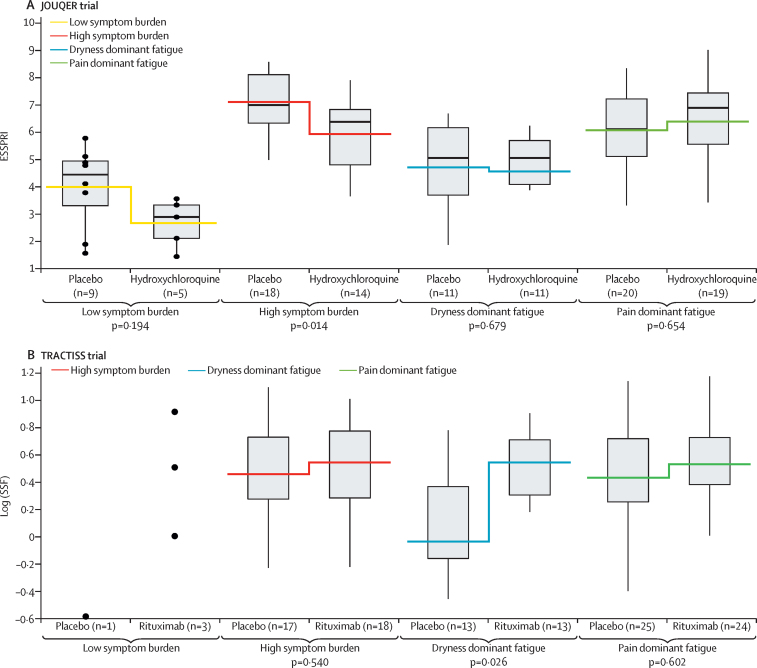
Findings: In the UKPSSR cohort (n=608), we identified four subgroups: Low symptom burden (LSB), high symptom burden (HSB), dryness dominant with fatigue (DDF), and pain dominant with fatigue (PDF). Significant differences in peripheral blood lymphocyte counts, anti-SSA and anti-SSB antibody positivity, as well as serum IgG, κ-free light chain, β2-microglobulin, and CXCL13 concentrations were observed between these subgroups, along with differentially expressed transcriptomic modules in peripheral blood. Similar findings were observed in the independent validation cohorts (n=396). Reanalysis of trial data stratifying patients into these subgroups suggested a treatment effect with hydroxychloroquine in the HSB subgroup and with rituximab in the DDF subgroup compared with placebo.
Interpretation: Stratification on the basis of patient-reported symptoms of patients with primary Sjögren's syndrome revealed distinct pathobiological endotypes with distinct responses to immunomodulatory treatments. Our data have important implications for clinical management, trial design, and therapeutic development. Similar stratification approaches might be useful for patients with other chronic immune-mediated diseases.
Funding: UK Medical Research Council, British Sjogren's Syndrome Association, French Ministry of Health, Arthritis Research UK, Foundation for Research in Rheumatology. VIDEO ABSTRACT.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures


References
-
- Fox RI. Sjogren's syndrome. Lancet. 2005;366:321–331. - PubMed
-
- Ng WF, Bowman SJ. Primary Sjogren's syndrome: too dry and too tired. Rheumatology. 2010;49:844–853. - PubMed
-
- Valtysdottir ST, Gudbjornsson B, Lindqvist U, Hallgren R, Hetta J. Anxiety and depression in patients with primary Sjogren's syndrome. J Rheumatol. 2000;27:165–169. - PubMed
-
- Westhoff G, Dorner T, Zink A. Fatigue and depression predict physician visits and work disability in women with primary Sjogren's syndrome: results from a cohort study. Rheumatology. 2012;51:262–269. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
