

Post-acute COVID-19 neuropsychiatric symptoms are not associated with ongoing nervous system injury
- PMID: 38229877
- PMCID: PMC10789589
- DOI: 10.1093/braincomms/fcad357
Post-acute COVID-19 neuropsychiatric symptoms are not associated with ongoing nervous system injury
Abstract
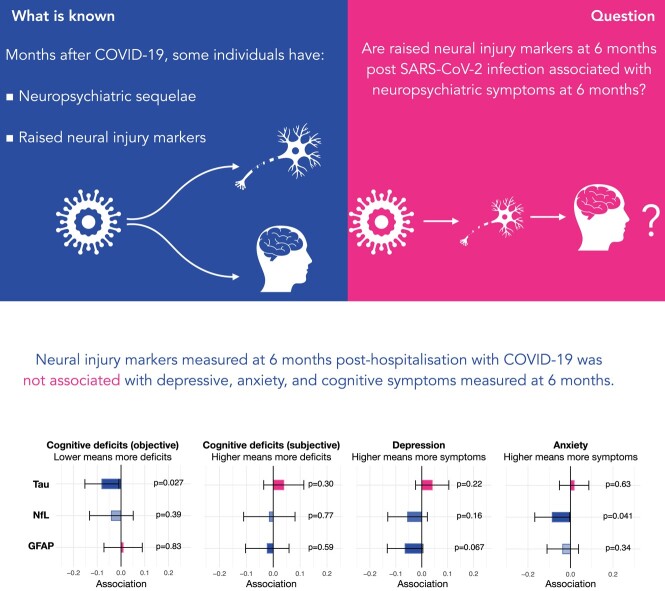
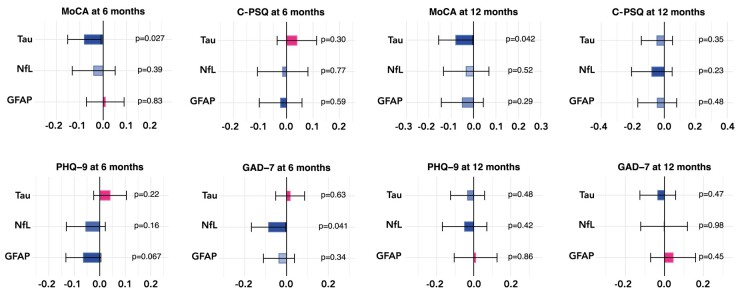
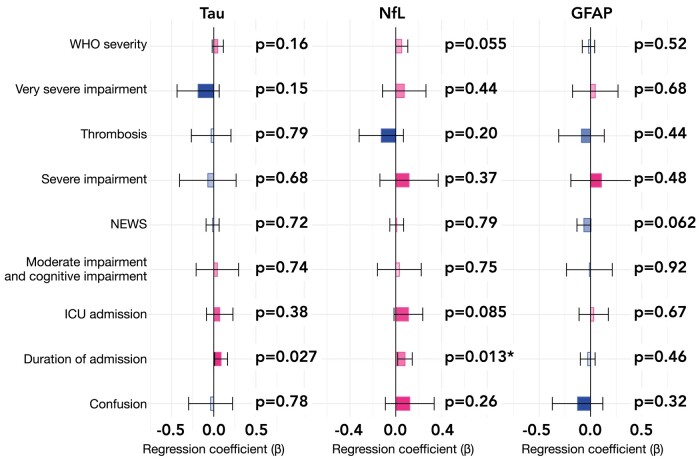
A proportion of patients infected with severe acute respiratory syndrome coronavirus 2 experience a range of neuropsychiatric symptoms months after infection, including cognitive deficits, depression and anxiety. The mechanisms underpinning such symptoms remain elusive. Recent research has demonstrated that nervous system injury can occur during COVID-19. Whether ongoing neural injury in the months after COVID-19 accounts for the ongoing or emergent neuropsychiatric symptoms is unclear. Within a large prospective cohort study of adult survivors who were hospitalized for severe acute respiratory syndrome coronavirus 2 infection, we analysed plasma markers of nervous system injury and astrocytic activation, measured 6 months post-infection: neurofilament light, glial fibrillary acidic protein and total tau protein. We assessed whether these markers were associated with the severity of the acute COVID-19 illness and with post-acute neuropsychiatric symptoms (as measured by the Patient Health Questionnaire for depression, the General Anxiety Disorder assessment for anxiety, the Montreal Cognitive Assessment for objective cognitive deficit and the cognitive items of the Patient Symptom Questionnaire for subjective cognitive deficit) at 6 months and 1 year post-hospital discharge from COVID-19. No robust associations were found between markers of nervous system injury and severity of acute COVID-19 (except for an association of small effect size between duration of admission and neurofilament light) nor with post-acute neuropsychiatric symptoms. These results suggest that ongoing neuropsychiatric symptoms are not due to ongoing neural injury.
Keywords: biomarkers; long COVID; neural injury.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
H.Z. has served at scientific advisory boards and/or as a consultant for Abbvie, Acumen, Alector, Alzinova, ALZPath, Annexon, Apellis, Artery Therapeutics, AZTherapies, CogRx, Denali, Eisai, Nervgen, Novo Nordisk, Passage Bio, Pinteon Therapeutics, Prothena, Red Abbey Labs, reMYND, Roche, Samumed, Siemens Healthineers, Triplet Therapeutics and Wave, has given lectures in symposia sponsored by Cellectricon, Fujirebio, Alzecure, Biogen and Roche, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program (outside submitted work). I.K. declares grant fundind and speaker fees from Novo Nordisk.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources