

Ultra-late response (> 24 weeks) to anti-CGRP monoclonal antibodies in migraine: a multicenter, prospective, observational study
- PMID: 38231271
- PMCID: PMC11055785
- DOI: 10.1007/s00415-023-12103-4
Ultra-late response (> 24 weeks) to anti-CGRP monoclonal antibodies in migraine: a multicenter, prospective, observational study
Erratum in
-
Correction to: Ultra-late response (> 24 weeks) to anti-CGRP monoclonal antibodies in migraine: a multicenter, prospective, observational study.J Neurol. 2024 May;271(5):2444-2445. doi: 10.1007/s00415-024-12287-3. J Neurol. 2024. PMID: 38564057 Free PMC article. No abstract available.
Abstract
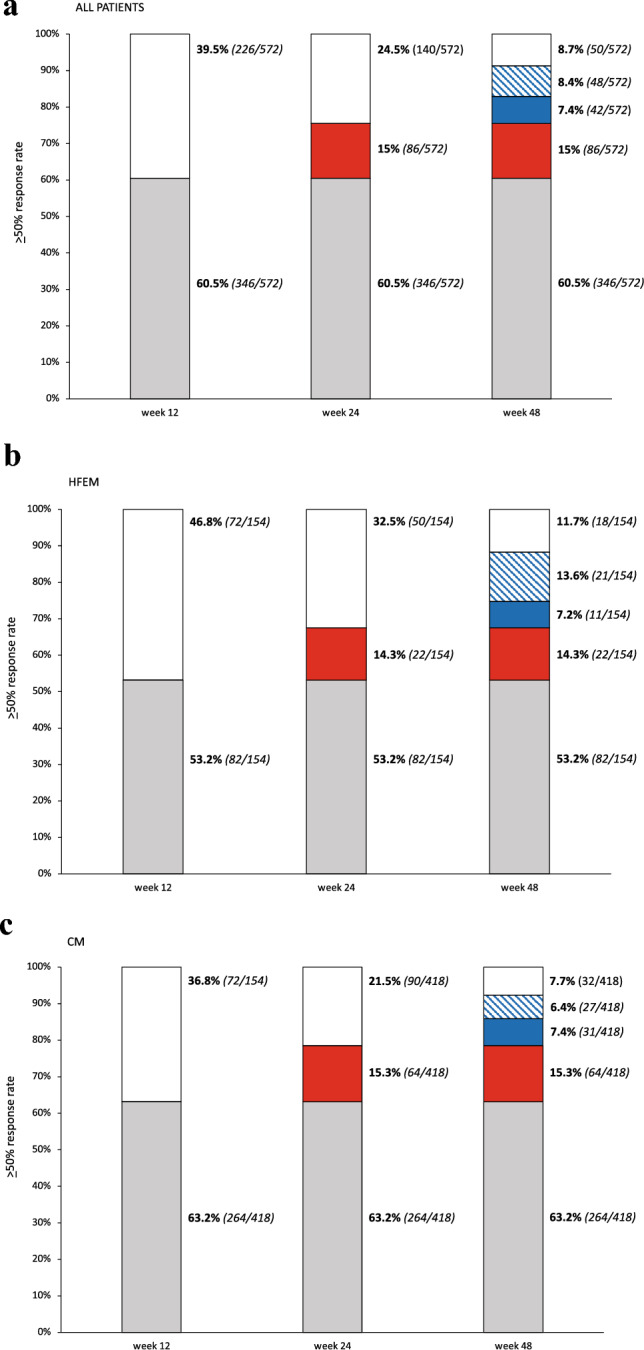
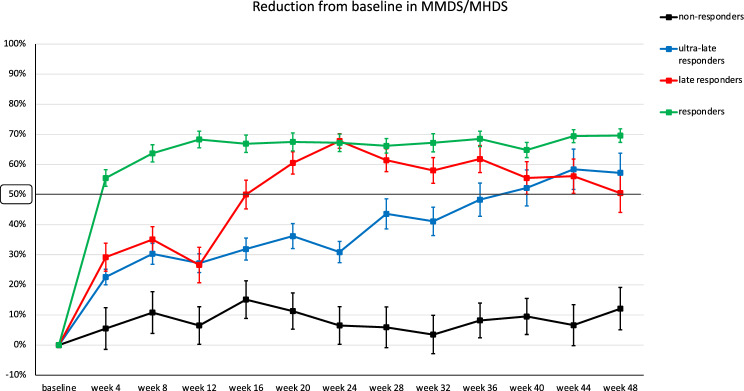
Objective: Nearly 60% of migraine patients treated with monoclonal antibodies (mAbs) targeting the calcitonin gene-related peptide (CGRP) pathway experience a ≥ 50% reduction in monthly migraine days (MMD) at 12 weeks compared to baseline (responders). However, approximately half of the patients not responding to anti-CGRP mAbs ≤ 12 weeks do respond ≤ 24 weeks (late responders). We assessed frequency and characteristics of patients responding to anti-CGRP mAbs only > 24 weeks (ultra-late responders).
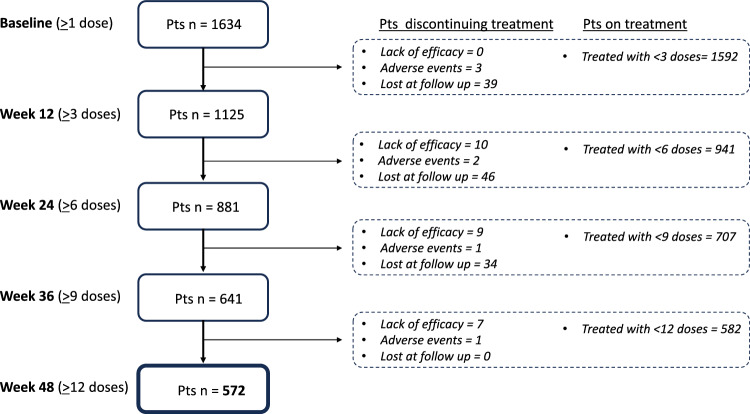
Methods: In this multicenter (n = 16), prospective, observational, real-life study, we enrolled all consecutive adults affected by high-frequency episodic migraine (HFEM: ≥ 8 days/month) or chronic migraine (CM), with ≥ 3 prior therapeutic failures, treated with any anti-CGRP mAbs for ≥ 48 weeks. We defined responders patients with a ≥ 50% response rate ≤ 12 weeks, late responders those with a ≥ 50% response rate ≤ 24 weeks, and ultra-late responders those achieving a ≥ 50% response only > 24 weeks.
Results: A total of 572 migraine patients completed ≥ 48 weeks of anti-CGRP mAbs treatment. Responders accounted for 60.5% (346/572), late responders for 15% (86/572), and ultra-late responders for 15.7% (90/572). Among ultra-late responders, 7.3% (42/572) maintained the ≥ 50% response rate across all subsequent time intervals (weeks 28, 32, 36, 40, 44, and 48) and were considered persistent ultra-late responders, while 8.4% (48/572) missed the ≥ 50% response rate at ≥ 1 subsequent time interval and were classified as fluctuating ultra-late responders. Fifty patients (8.7%) did not respond at any time interval ≤ 48 weeks. Ultra-late responders differed from responders for higher BMI (p = 0.033), longer duration of medication overuse (p < 0.001), lower NRS (p = 0.017) and HIT-6 scores (p = 0.002), higher frequency of dopaminergic symptoms (p = 0.002), less common unilateral pain-either alone (p = 0.010) or in combination with UAS (p = 0.023), allodynia (p = 0.043), or UAS and allodynia (p = 0.012)-a higher number of comorbidities (p = 0.012), psychiatric comorbidities (p = 0.010) and a higher proportion of patients with ≥ 1 comorbidity (p = 0.020).
Conclusion: Two-thirds of patients not responding to anti-CGRP mAbs ≤ 24 weeks do respond later, while non-responders ≤ 48 weeks are quite rare (8.7%). These findings suggest to rethink the duration of migraine prophylaxis and the definition of resistant and refractory migraine, currently based on the response after 2-3 months of treatment.
Keywords: Anti-CGRP mAbs; Late response; Migraine; Real-life; Responder; Treatment; Ultra-late response.
© 2024. The Author(s).
Conflict of interest statement
Piero Barbanti reports personal compensation for consulting, serving on a scientific advisory board, speaking, research support, collaborated for clinical trials, or other activities with Abbvie, Alder, Allergan, Amgen, Angelini, Assosalute, Bayer, Biohaven, ElectroCore, Eli-Lilly, Fondazione Ricerca e Salute, GSK, Lundbeck, Lusofarmaco, 1MED, MSD, New Penta, Noema Pharma, Novartis, Pfizer, Stx-Med, Teva, Visufarma, Zambon and serves as President with Italian Association of Headache Sufferers. Cinzia Aurilia received travel grants from Eli-Lilly, FB-Health, Lusofarmaco and Teva, honoraria from Novartis, Eli-Lilly and Teva; Gabriella Egeo received travel grants and honoraria from Eli-Lilly, Novartis, New Penta and Ecupharma; Florindo d’Onofrio received travel grant, honoraria as a speaker or for participating in advisory boards from Novartis, Teva, Neopharmed Gentili, Qbgroup srl, K link srl and Eli-Lilly; Paola Torelli received travel grant, honoraria as a speaker, or for participating in advisory boards from Novartis, Teva, Eli Lilly, and Allergan; Cinzia Finocchi received grants and honoraria from Novartis, Eli Lilly, TEVA, AIM group; Sabina Cevoli received honoraria for speaker panels from Teva and Novartis; Maurizio Zucco received travel grants and honoraria from Novartis; Bruno Colombo received travel grants, honoraria for advisory boards, speaker panels or investigation studies from Novartis, Teva, Lilly e Lusofarmaco; Valentina Favoni received honoraria as speaker or for participating in advisory boards from Ely-Lilly, Novartis and Teva; Licia Grazzi received consultancy and advisory fees or honoraria for investigation studies from Allergan, Electrocore LLC, Novartis, Ely-Lilly and Teva; Frediani Fabio received honoraria as speaker or for participating in advisory boards from Novartis, Teva and Eli-Lilly; Claudia Altamura received honoraria for speaker panels from Novartis and Teva; Massimo Filippi is Editor-in-Chief of the Journal of Neurology; received compensation for consulting services and/or speaking activities from Bayer, Biogen Idec, Merck-Serono, Novartis, Roche, Sanofi Genzyme, Takeda, and Teva; and receives research support from Biogen Idec, Merck-Serono, Novartis, Roche, Teva, Italian Ministry of Health, Fondazione Italiana Sclerosi Multipla, and ARiSLA (Fondazione Italiana di Ricerca per la SLA); Fabrizio Vernieri received travel grants, honoraria for advisory boards, speaker panels, or clinical investigation studies from Allergan, Eli-Lilly, Novartis, and Teva; Stefania Proietti, Marco Aguggia, Davide Bertuzzo, Michele Trimboli, Ilaria Cetta, Monica Laura Bandettini di Poggio, Giulia Fiorentini, Bianca Orlando, Laura Di Clemente, Antonio Salerno, Antonio Carnevale, Micaela Robotti and Stefano Bonassi have no disclosures to declare.
Figures
References
-
- Lipton RB, Nicholson RA, Reed ML, Araujo AB, Jaffe DH, Faries DE, Buse DC, Shapiro RE, Ashina S, Cambron-Mellott MJ, Rowland JC, Pearlman EM. Diagnosis, consultation, treatment, and impact of migraine in the US: Results of the OVERCOME (US) study. Headache. 2022;62(2):122–140. doi: 10.1111/head.14259. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
