

Acute evacuation of 54 intracerebral hematomas (aICH) during the microsurgical clipping of a ruptured middle cerebral artery bifurcation aneurysm-illustration of the individual clinical courses and outcomes with a serial brain CT/MRI panel until 12 months
- PMID: 38231317
- PMCID: PMC10794262
- DOI: 10.1007/s00701-024-05902-9
Acute evacuation of 54 intracerebral hematomas (aICH) during the microsurgical clipping of a ruptured middle cerebral artery bifurcation aneurysm-illustration of the individual clinical courses and outcomes with a serial brain CT/MRI panel until 12 months
Abstract
Purpose: In aneurysmal intracerebral hemorrhage (aICH), our review showed the lack of the patient's individual (i) timeline panels and (ii) serial brain CT/MRI slice panels through the aICH evacuation and neurointensive care until the final brain tissue outcome.
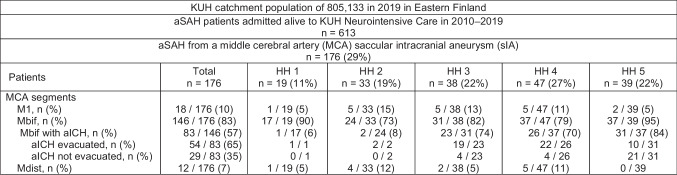
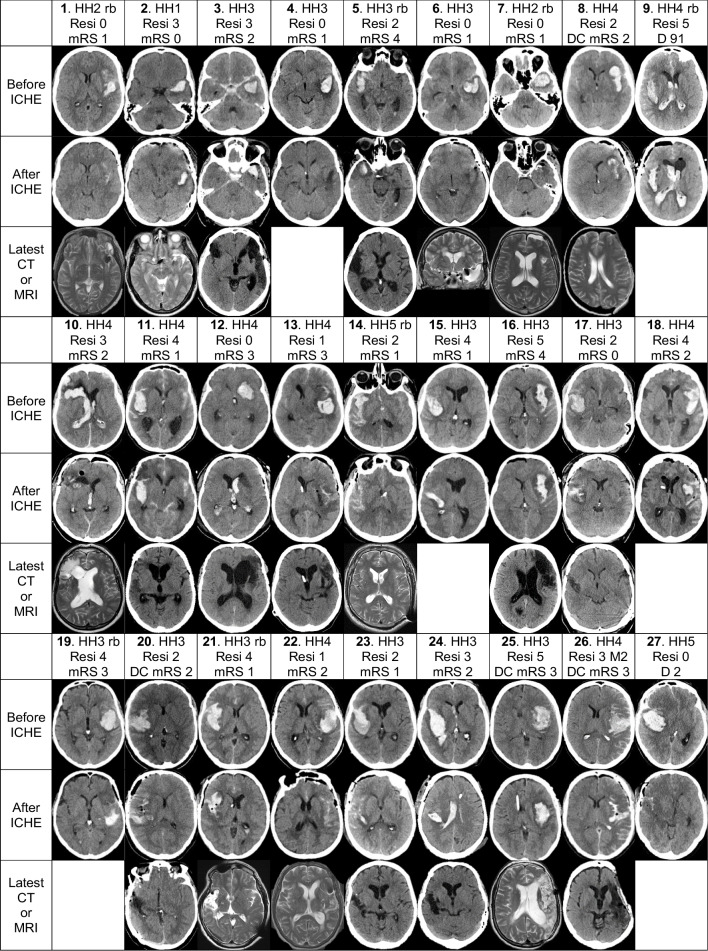
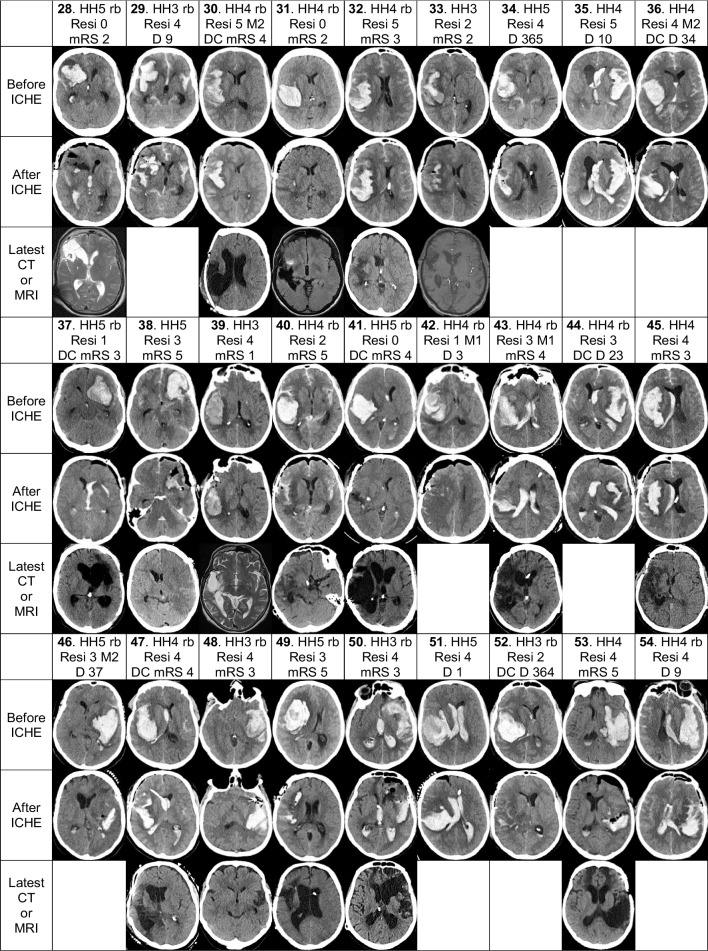
Methods: Our retrospective cohort consists of 54 consecutive aICH patients from a defined population who acutely underwent the clipping of a middle cerebral artery bifurcation saccular aneurysm (Mbif sIA) with the aICH evacuation at Kuopio University Hospital (KUH) from 2010 to 2019. We constructed the patient's individual timeline panels since the emergency call and serial brain CT/MRI slice panels through the aICH evacuation and neurointensive care until the final brain tissue outcome. The patients were indicated by numbers (1.-54.) in the pseudonymized panels, tables, results, and discussion.
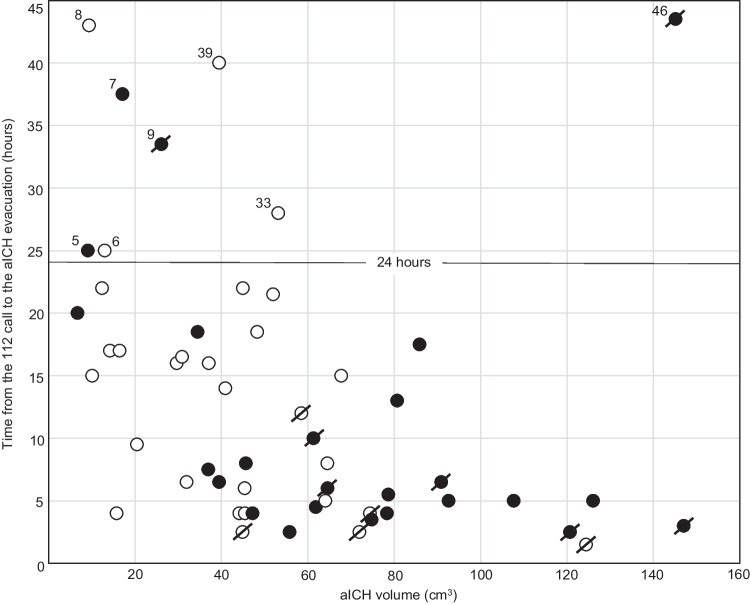
Results: The aICH volumes on KUH admission (median 46 cm3) plotted against the time from the emergency call to the evacuation (median 8 hours) associated significantly with the rebleeds (n=25) and the deaths (n=12). The serial CT/MRI slice panels illustrated the aICHs, intraventricular hemorrhages (aIVHs), residuals after the aICH evacuations, perihematomal edema (PHE), delayed cerebral injury (DCI), and in the 42 survivors, the clinical outcome (mRS) and the brain tissue outcome.
Conclusions: Regarding aICH evacuations, serial brain CT/MRI panels present more information than words, figures, and graphs. Re-bleeds associated with larger aICH volumes and worse outcomes. Swift logistics until the sIA occlusion with aICH evacuation is required, also in duty hours and weekends. Intraoperative CT is needed to illustrate the degree of aICH evacuation. PHE may evoke uncontrollable intracranial pressure (ICP) in spite of the acute aICH volume reduction.
Keywords: Aneurysmal intracerebral hematoma; Brain tissue outcome; EMS Emergency medical services; Individual serial brain imaging panel; Microsurgical evacuation and clipping; Perihematomal edema.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Autio AH, Paavola J, Tervonen J, Lång M, Huuskonen TJ, Huttunen J, Kärkkäinen V, von Und Z, Fraunberg M, Lindgren AE, Koivisto T, Kurola J, Jääskeläinen JE, Kämäräinen OP (2023) Should individual timeline and serial CT/MRI panels of all patients be presented in acute brain insult cohorts? A pilot study of 45 patients with decompressive craniectomy after aneurysmal subarachnoid hemorrhage. Acta Neurochir. 10.1007/s00701-022-05473-7 - PMC - PubMed
-
- Autio AH, Paavola J, Tervonen J, Lång M, Huuskonen TJ, Huttunen J, Kärkkäinen V, von Und Z, Fraunberg M, Lindgren AE, Koivisto T, Jääskeläinen JE, Kämäräinen OP (2021) Clinical condition of 120 patients alive at 3 years after poor-grade aneurysmal subarachnoid hemorrhage. Acta Neurochir. 10.1007/s00701-021-04725-2 - PMC - PubMed
-
- Baldvinsdóttir B, Kronvall E, Ronne-Engström E, Enblad P, Lindvall P, Aineskog H, Friðriksson S, Klurfan P, Svensson M, Alpkvist P, Hillman J, Eneling J, Nilsson OG (2023) Adverse events associated with microsurgial treatment for ruptured intracerebral aneurysms: a prospective nationwide study on subarachnoid haemorrhage in Sweden. J Neurol Neurosurg Psychiatry. 10.1136/jnnp-2022-330982 - PubMed
-
- Bohnstedt BN, Nguyen HS, Kulwin CG, Shoja MM, Helbig GM, Leipzig TJ, Payner TD, Cohen-Gadol AA (2013) Outcomes for clip ligation and hematoma evacuation associated with 102 patients with ruptured middle cerebral artery aneurysms. World Neurosurg. 10.1016/j.wneu.2012.03.008 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
