

Position Statement on the Use of Myocardial Strain in Cardiology Routines by the Brazilian Society of Cardiology's Department Of Cardiovascular Imaging - 2023
- PMID: 38232246
- PMCID: PMC10789373
- DOI: 10.36660/abc.20230646
Position Statement on the Use of Myocardial Strain in Cardiology Routines by the Brazilian Society of Cardiology's Department Of Cardiovascular Imaging - 2023
Abstract
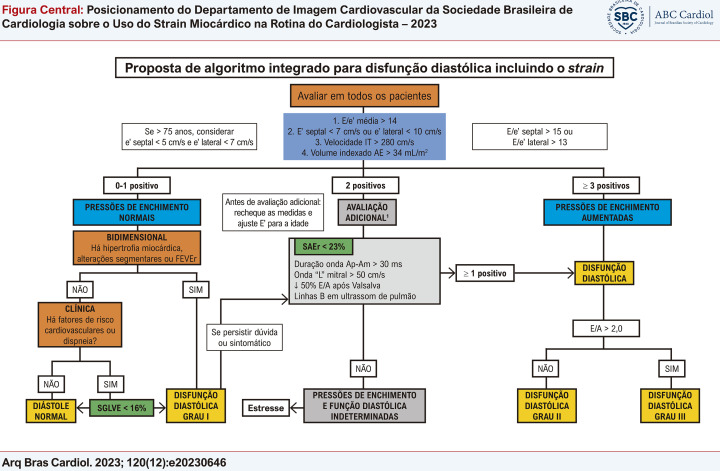
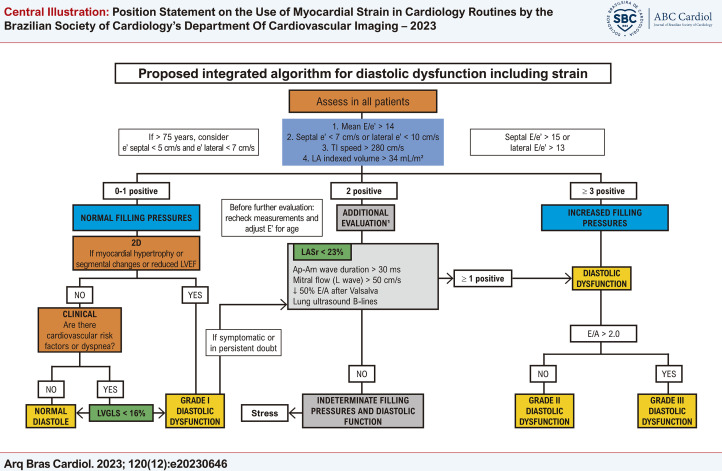
Central Illustration : Position Statement on the Use of Myocardial Strain in Cardiology Routines by the Brazilian Society of Cardiology's Department Of Cardiovascular Imaging - 2023 Proposal for including strain in the integrated diastolic function assessment algorithm, adapted from Nagueh et al.67 Am: mitral A-wave duration; Ap: reverse pulmonary A-wave duration; DD: diastolic dysfunction; LA: left atrium; LASr: LA strain reserve; LVGLS: left ventricular global longitudinal strain; TI: tricuspid insufficiency. Confirm concentric remodeling with LVGLS. In LVEF, mitral E wave deceleration time < 160 ms and pulmonary S-wave < D-wave are also parameters of increased filling pressure. This algorithm does not apply to patients with atrial fibrillation (AF), mitral annulus calcification, > mild mitral valve disease, left bundle branch block, paced rhythm, prosthetic valves, or severe primary pulmonary hypertension.
Figura Central : Posicionamento do Departamento de Imagem Cardiovascular da Sociedade Brasileira de Cardiologia sobre o Uso do Strain Miocárdico na Rotina do Cardiologista – 2023 Proposta de inclusão do strain no algoritmo integrado de avaliação da função diastólica, adaptado e traduzido de Nagueh et al. 67 AE: átrio esquerdo; Ap: duração da onda A reversa pulmonar; Am: duração da onda A mitral; DD: disfunção diastólica; FEVEr: fração de ejeção do ventrículo esquerdo reduzida; IT: insuficiência tricúspide; SAEr: strain do AE de reservatório; SLGVE: strain longitudinal global do ventrículo esquerdo. Se remodelamento concêntrico, confirmar com SLGVE. Na presença de FEVEr, tempo de desaceleração da onda E mitral (TDE) < 160 ms e onda S < D pulmonar também são parâmetros de pressão de enchimento aumentada. Esse algoritmo não se aplica a pacientes com fibrilação atrial (FA), calcificação do anel mitral ou valvopatia mitral maior que discreta, bloqueio de ramo esquerdo (BRE), ritmo de marca-passo, próteses valvares ou hipertensão pulmonar (HP) primária grave.
Figures


References
-
- Loizou CP, Pattichis CS, D’Hooge J. Handbook of Speckle Filtering and Tracking in Cardiovascular Ultrasound Imaging and Video. London: The Institution of Engineering and Technology; 2018.
-
- Tressino CG, Hortegal RA, Momesso M, Barretto RBM, Le Bihan D. Como eu Faço: Avaliação do Strain do Ventrículo Esquerdo. Arq Bras Cardiol: Imagem Cardiovasc. 2020;33(4):ecom15. doi: 10.47593/2675-312X/20203304ecom15. - DOI
-
- Hortegal R, Abensur H. Strain Echocardiography in Patients with Diastolic Dysfunction and Preserved Ejection Fraction: Are We Ready? Arq Bras Cardiol: Imagem Cardiovasc. 2017;30(4):132–139. doi: 10.5935/2318-8219.20170034. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
