

Interventions Performed in Children With Immunocompromised Conditions in the Pediatric Intensive Care Unit Within 48 Hours of Death
- PMID: 38232707
- PMCID: PMC11971613
- DOI: 10.1089/jpm.2023.0400
Interventions Performed in Children With Immunocompromised Conditions in the Pediatric Intensive Care Unit Within 48 Hours of Death
Abstract
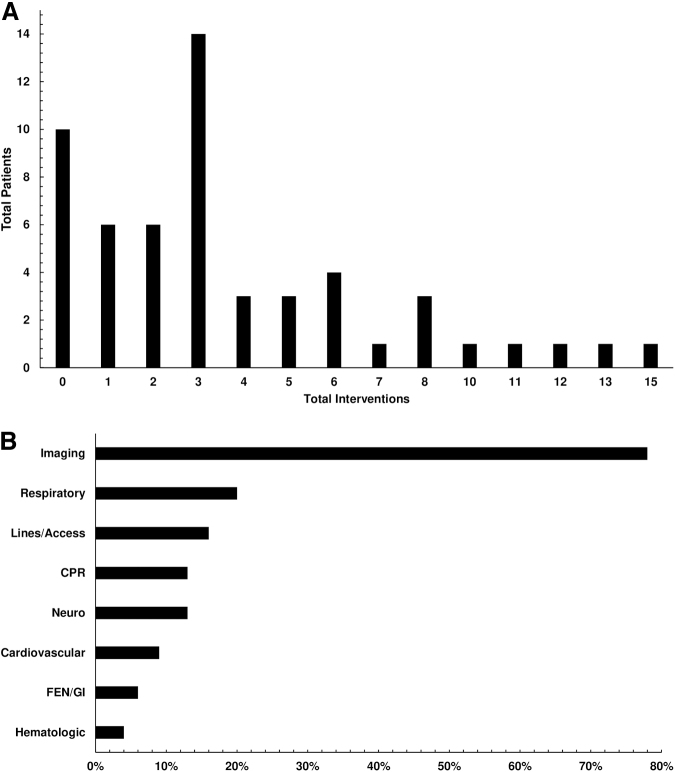
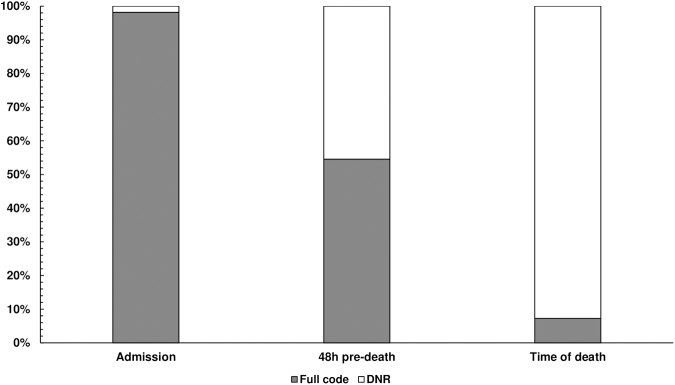
Background: Understanding interventions preceding death in children with immunocompromised conditions is important to ensure a peaceful and dignified perideath experience. The aim of this study was to describe the number of interventions performed in the pediatric intensive care unit (PICU) within the 48 hours before death in this population. Methods: This was a single-center, retrospective cohort study of all children with an underlying oncologic, hematologic, or immunologic diagnosis admitted to the PICU for at least 72 hours between 2014 and 2021. Medical records were reviewed for interventions within 48 hours preceding death and for palliative care involvement. Interventions were defined as new or escalations in respiratory support, cardiopulmonary resuscitation (CPR), vascular access, drains, and radiographic studies. Associations were evaluated using simple logistic regression. Results: A total of 55 patients were included in this study. The predominant PICU admission diagnoses were respiratory (51%), followed by shock (25%), and neurologic diagnoses (9%). These predominant diagnoses were similar perideath. At PICU admission, only 1 patient had a do-not-resuscitate (DNR) order. Forty-six percent had a DNR order 48 hours preceding death, and 91% had DNR orders in place at time of death. During the 48-hour period preceding death, 80% of children received at least one intervention. Radiographic studies were the most common, used in 78% of children, followed by respiratory (20%), vascular (16%), CPR (13%), and drain placement (7%). Palliative care was involved in 38% of cases and was associated with a decrease in the number of radiologic interventions (p = 0.028) and CPR (p = 0.026). Conclusions: Children in the PICU with underlying immunocompromised conditions frequently receive interventions within the 48-hour period preceding death. Palliative care involvement was associated with fewer radiographic studies and fewer occurrences of CPR. The impact of interventions on the dying experience warrants further investigation.
Keywords: critical care; immunocompromised host; neoplasms; palliative care; pediatrics; terminal care.
Figures
Similar articles
-
Changes in Clinical Course Before and After Do-Not-Resuscitate Order Placement in a Pediatric Intensive Care Unit Setting.J Palliat Med. 2021 Jan;24(1):107-111. doi: 10.1089/jpm.2019.0572. Epub 2020 Apr 3. J Palliat Med. 2021. PMID: 32250188
-
Death and Dying in Hospitalized Pediatric Patients: A Prospective Multicenter, Multinational Study.J Palliat Med. 2022 Feb;25(2):227-233. doi: 10.1089/jpm.2021.0205. Epub 2021 Nov 30. J Palliat Med. 2022. PMID: 34847737
-
Do not resuscitate orders in a Saudi pediatric intensive care unit.Saudi Med J. 2014 Jun;35(6):561-5. Saudi Med J. 2014. PMID: 24888654
-
Efficacy and outcome of intensive care in pediatric oncologic patients.Crit Care Med. 2001 Dec;29(12):2276-80. doi: 10.1097/00003246-200112000-00007. Crit Care Med. 2001. PMID: 11801824
-
Withdrawal and limitation of life-sustaining treatments in a paediatric intensive care unit and review of the literature.J Paediatr Child Health. 2008 Jul-Aug;44(7-8):404-8. doi: 10.1111/j.1440-1754.2008.01353.x. J Paediatr Child Health. 2008. PMID: 18638332 Review.
References
-
- Rubenfeld GD, Curtis JR. End-of-life care in the intensive care unit: A research agenda. Crit Care Med 2001;10:2001–2006. - PubMed
-
- Forsner M, Mattson J. Caring for dying children in the pediatric intensive care unit, nurses and parents' perspective. J Complement Altern Med 2019;1.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
