

Racial and skin color mediated disparities in pulse oximetry in infants and young children
- PMID: 38233229
- PMCID: PMC11139570
- DOI: 10.1016/j.prrv.2023.12.006
Racial and skin color mediated disparities in pulse oximetry in infants and young children
Abstract
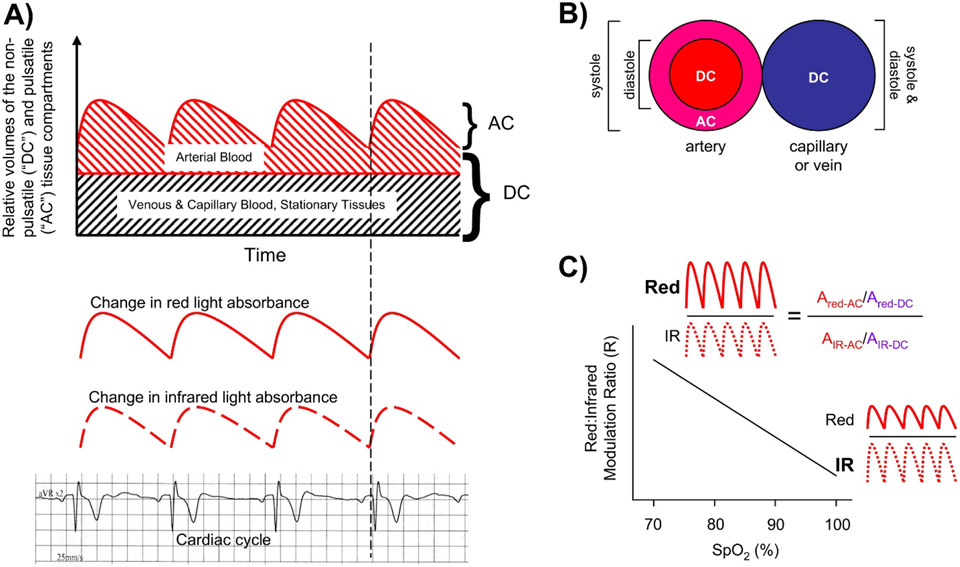
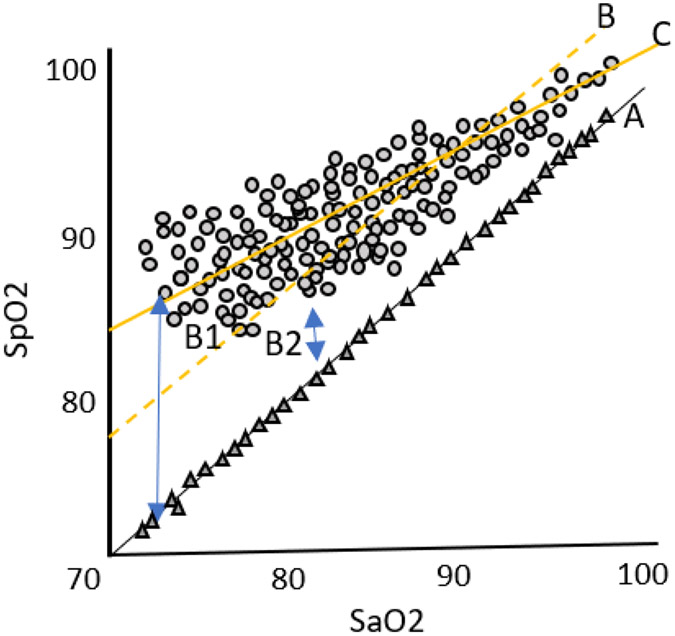
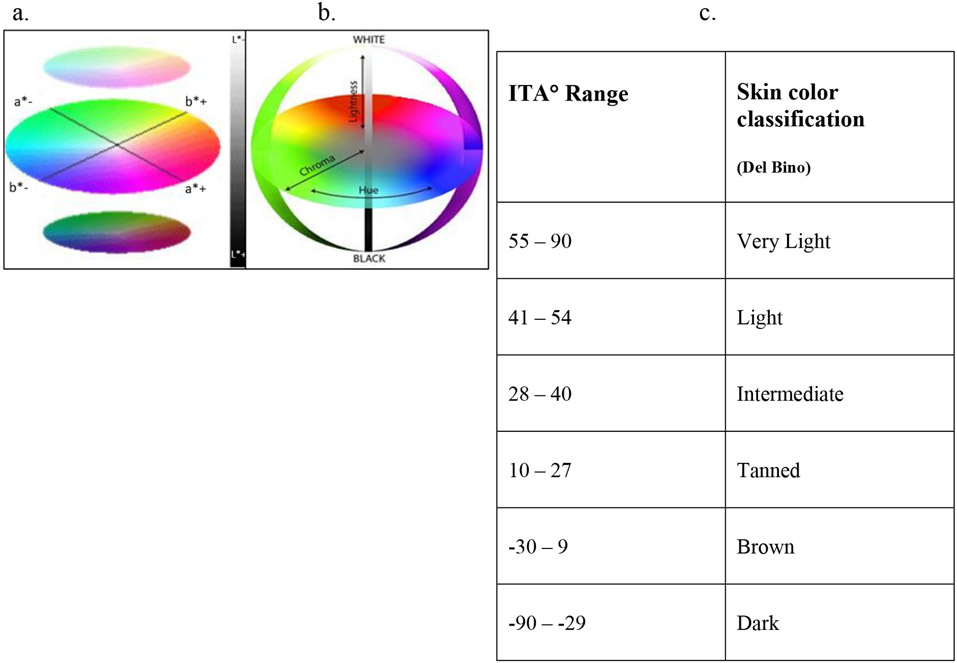
Race-based and skin pigmentation-related inaccuracies in pulse oximetry have recently been highlighted in several large electronic health record-based retrospective cohort studies across diverse patient populations and healthcare settings. Overestimation of oxygen saturation by pulse oximeters, particularly in hypoxic states, is disparately higher in Black compared to other racial groups. Compared to adult literature, pediatric studies are relatively few and mostly reliant on birth certificates or maternal race-based classification of comparison groups. Neonates, infants, and young children are particularly susceptible to the adverse life-long consequences of hypoxia and hyperoxia. Successful neonatal resuscitation, precise monitoring of preterm and term neonates with predominantly lung pathology, screening for congenital heart defects, and critical decisions on home oxygen, ventilator support and medication therapies, are only a few examples of situations that are highly reliant on the accuracy of pulse oximetry. Undetected hypoxia, especially if systematically different in certain racial groups may delay appropriate therapies and may further perpetuate health care disparities. The role of biological factors that may differ between racial groups, particularly skin pigmentation that may contribute to biased pulse oximeter readings needs further evaluation. Developmental and maturational changes in skin physiology and pigmentation, and its interaction with the operating principles of pulse oximetry need further study. Importantly, clinicians should recognize the limitations of pulse oximetry and use additional objective measures of oxygenation (like co-oximetry measured arterial oxygen saturation) where hypoxia is a concern.
Keywords: Disparity; Infants; Oxygen; Pulse Oximeter; Race; Skin Pigmentation.
Copyright © 2024 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Low Perfusion and Missed Diagnosis of Hypoxemia by Pulse Oximetry in Darkly Pigmented Skin: A Prospective Study.Anesth Analg. 2024 Mar 1;138(3):552-561. doi: 10.1213/ANE.0000000000006755. Epub 2023 Dec 18. Anesth Analg. 2024. PMID: 38109495
-
Disparities in Hypoxemia Detection by Pulse Oximetry Across Self-Identified Racial Groups and Associations With Clinical Outcomes.Crit Care Med. 2022 Feb 1;50(2):204-211. doi: 10.1097/CCM.0000000000005394. Crit Care Med. 2022. PMID: 35100193 Free PMC article.
-
Racial Disparity in Oxygen Saturation Measurements by Pulse Oximetry: Evidence and Implications.Ann Am Thorac Soc. 2022 Dec;19(12):1951-1964. doi: 10.1513/AnnalsATS.202203-270CME. Ann Am Thorac Soc. 2022. PMID: 36166259 Review.
-
Performance of pulse oximeters as a function of race compared to skin pigmentation: a single center retrospective study.J Clin Monit Comput. 2025 Feb;39(1):119-125. doi: 10.1007/s10877-024-01211-9. Epub 2024 Aug 28. J Clin Monit Comput. 2025. PMID: 39196478 Free PMC article.
-
Impacts of Skin Color and Hypoxemia on Noninvasive Assessment of Peripheral Blood Oxygen Saturation: A Scoping Review.Cureus. 2023 Sep 27;15(9):e46078. doi: 10.7759/cureus.46078. eCollection 2023 Sep. Cureus. 2023. PMID: 37900526 Free PMC article.
Cited by
-
2025 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association.Circulation. 2025 Feb 25;151(8):e41-e660. doi: 10.1161/CIR.0000000000001303. Epub 2025 Jan 27. Circulation. 2025. PMID: 39866113 Review.
-
Oxygen saturation targets in neonatal care: A narrative review.Early Hum Dev. 2024 Dec;199:106134. doi: 10.1016/j.earlhumdev.2024.106134. Epub 2024 Oct 28. Early Hum Dev. 2024. PMID: 39481153 Review.
-
Comparison of the oxygenation index and the oxygen saturation index as clinical indicators for neonatal ECMO.Front Pediatr. 2025 Jun 24;13:1586985. doi: 10.3389/fped.2025.1586985. eCollection 2025. Front Pediatr. 2025. PMID: 40630719 Free PMC article.
-
Objective Assessment and Quantification of Skin Color and Melanin in Neonates and Infants: A State-Of-The-Art Review.Pediatr Dermatol. 2025 May-Jun;42(3):447-456. doi: 10.1111/pde.15902. Epub 2025 Mar 7. Pediatr Dermatol. 2025. PMID: 40051289 Review.
-
Color outside the lines: rethinking Apgar scores for equity.Pediatr Res. 2024 Nov 11. doi: 10.1038/s41390-024-03701-7. Online ahead of print. Pediatr Res. 2024. PMID: 39528744 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
