

Management of frontal sinus trauma: a retrospective study of surgical interventions and complications
- PMID: 38233722
- PMCID: PMC10794673
- DOI: 10.1186/s40902-024-00414-z
Management of frontal sinus trauma: a retrospective study of surgical interventions and complications
Abstract
Background: Frontal sinus injuries are relatively rare among facial bone traumas. Without proper treatment, they can lead to fatal intracranial complications, including meningitis or brain abscesses, as well as aesthetic and functional sequelae. The management of frontal sinus injuries remains controversial, with various treatment methods and outcomes being reported. This article describes the clinical characteristics, surgical methods, and outcomes among 17 patients who underwent surgery for frontal sinus injury and related complications.
Case presentation: We retrospectively included 17 patients who underwent surgery for frontal sinus injury and its related complications at the Kangwon National University Hospital between July 2010 and September 2021. Among them, six underwent simple open reduction and fixation of the anterior wall, eight underwent sinus obliteration, and three underwent cranialization. Two patients who underwent sinus obliteration died due to infection-related complications. The patient who underwent cranialization reported experiencing chronic headache and expressed dissatisfaction regarding the esthetic outcomes of the forehead. Except for these three patients, the other patients achieved satisfactory esthetic and functional recovery.
Conclusion: Active surgical management of frontal sinus injuries is often required owing to the various complications caused by these injuries; however, several factors, including the fracture type, clinical presentation, related craniomaxillofacial injury, and medical history, should be considered while formulating the treatment plan. Surgical treatment through the opening of the frontal sinus should be actively considered in patients with severely damaged posterior wall fractures and those at risk of developing infection.
Keywords: Complications; Cranialization; Frontal sinus fracture; Infection; Obliteration.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
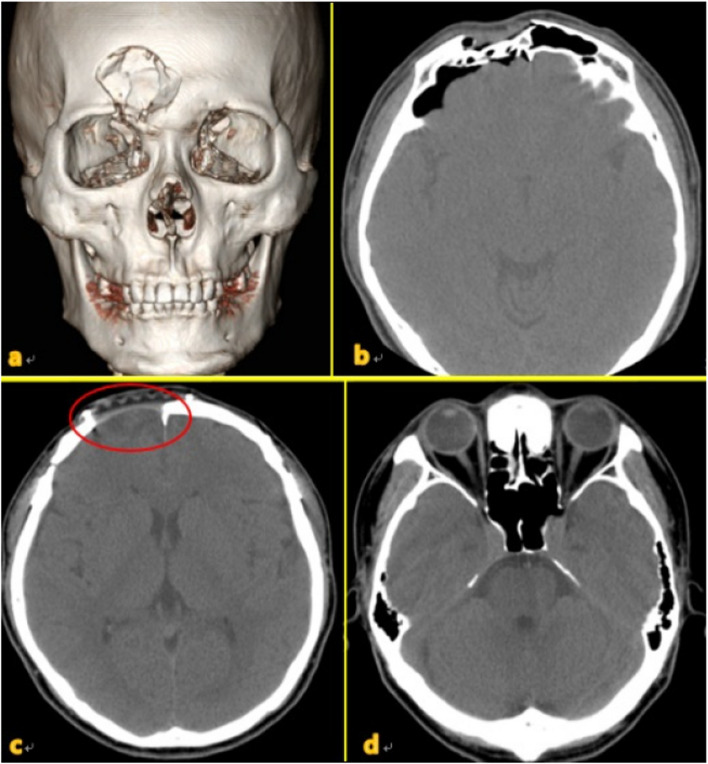
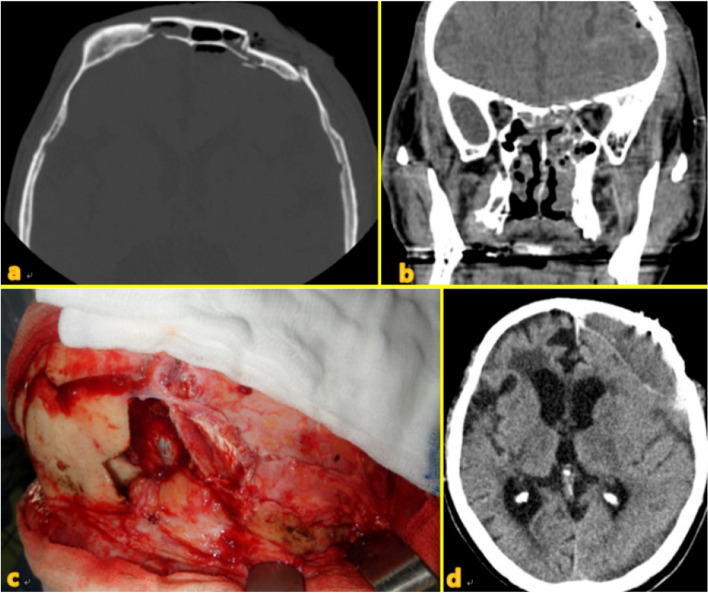
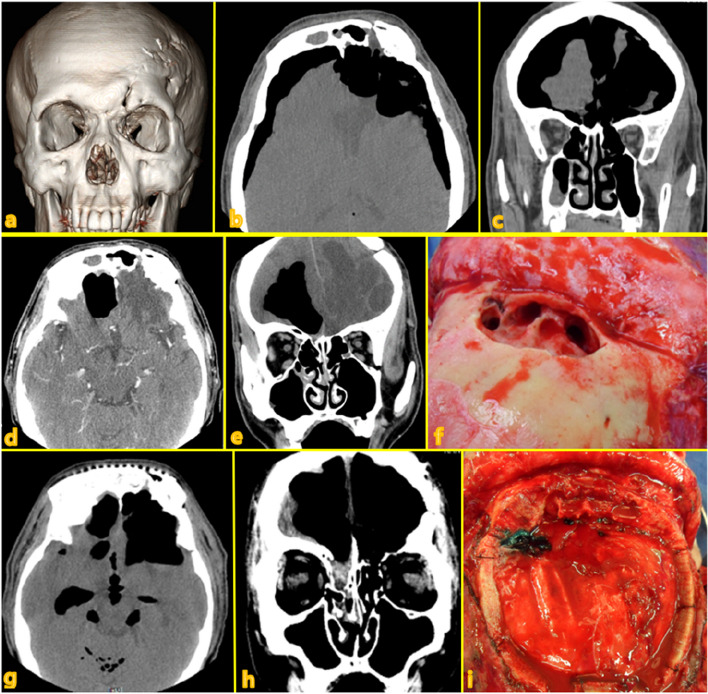
Figures
Similar articles
-
A protocol for the management of frontal sinus fractures emphasizing sinus preservation.J Oral Maxillofac Surg. 2007 May;65(5):825-39. doi: 10.1016/j.joms.2006.05.058. J Oral Maxillofac Surg. 2007. PMID: 17448829
-
A 10-year review of frontal sinus fractures: clinical outcomes of conservative management of posterior table fractures.Plast Reconstr Surg. 2012 Aug;130(2):399-406. doi: 10.1097/PRS.0b013e3182589d91. Plast Reconstr Surg. 2012. PMID: 22495212
-
Frontal Bone Fractures and Frontal Sinus Injuries: Treatment Paradigms.Ann Maxillofac Surg. 2019 Jul-Dec;9(2):261-282. doi: 10.4103/ams.ams_151_19. Ann Maxillofac Surg. 2019. PMID: 31909005 Free PMC article.
-
State of the art in craniomaxillofacial trauma: frontal sinus.Curr Opin Otolaryngol Head Neck Surg. 2008 Aug;16(4):381-6. doi: 10.1097/MOO.0b013e328308672c. Curr Opin Otolaryngol Head Neck Surg. 2008. PMID: 18626259 Review.
-
Trauma in Facial Plastic Surgery: Frontal Sinus Fractures.Facial Plast Surg Clin North Am. 2017 Nov;25(4):503-511. doi: 10.1016/j.fsc.2017.06.004. Facial Plast Surg Clin North Am. 2017. PMID: 28941504 Review.
Cited by
-
Guided Frontal Sinus Osteotomy: A Pilot Study of a Digital Protocol for "In-House" Manufacturing Surgical Cutting Guides.J Clin Med. 2025 May 1;14(9):3141. doi: 10.3390/jcm14093141. J Clin Med. 2025. PMID: 40364172 Free PMC article.
References
-
- Nahum AM. The biomechanics of maxillofacial trauma. Clin Plast Surg. 1975;2:59–64. - PubMed
-
- Gossman DG, Archer SM, Arosarena O. Management of frontal sinus fractures: a review of 96 cases. Laryngoscope. 2006;116:1357–1362. - PubMed
-
- Bell RB, Dierks EJ, Brar P, Potter JK, Potter BE. A protocol for the management of frontal sinus fractures emphasizing sinus preservation. J Oral Maxillofac Surg. 2007;65:825–839. - PubMed
-
- Gerbino G, Roccia F, Benech A, Caldarelli C. Analysis of 158 frontal sinus fractures: current surgical management and complications. J Craniomaxillofac Surg. 2000;28:133–139. - PubMed
LinkOut - more resources
Full Text Sources