

How does hospital organisation influence the use of caesarean sections in low- and middle-income countries? A cross-sectional survey in Argentina, Burkina Faso, Thailand and Vietnam for the QUALI-DEC project
- PMID: 38233792
- PMCID: PMC10792793
- DOI: 10.1186/s12884-024-06257-w
How does hospital organisation influence the use of caesarean sections in low- and middle-income countries? A cross-sectional survey in Argentina, Burkina Faso, Thailand and Vietnam for the QUALI-DEC project
Abstract
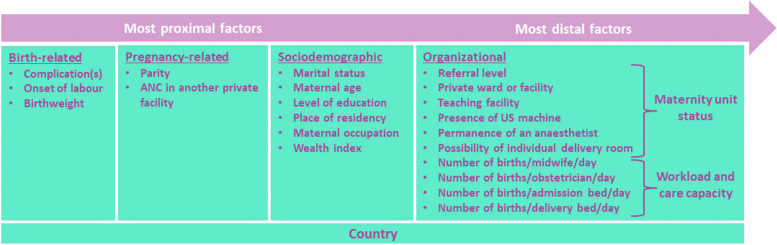
Background: Improving the understanding of non-clinical factors that lead to the increasing caesarean section (CS) rates in many low- and middle-income countries is currently necessary to meet the challenge of implementing effective interventions in hospitals to reverse the trend. The objective of this study was to study the influence of organizational factors on the CS use in Argentina, Vietnam, Thailand and Burkina Faso.
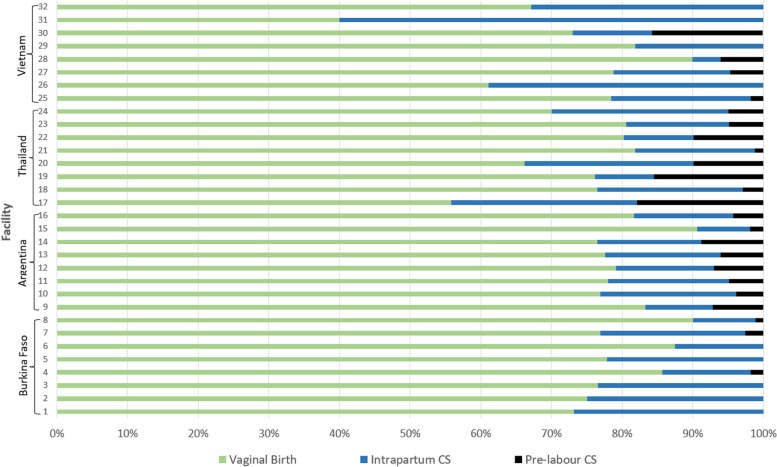
Methods: A cross-sectional hospital-based postpartum survey was conducted in 32 hospitals (8 per country). We selected women with no potential medical need for CS among a random sample of women who delivered at each of the participating facilities during the data collection period. We used multilevel multivariable logistic regression to analyse the association between CS use and organizational factors, adjusted on women's characteristics.
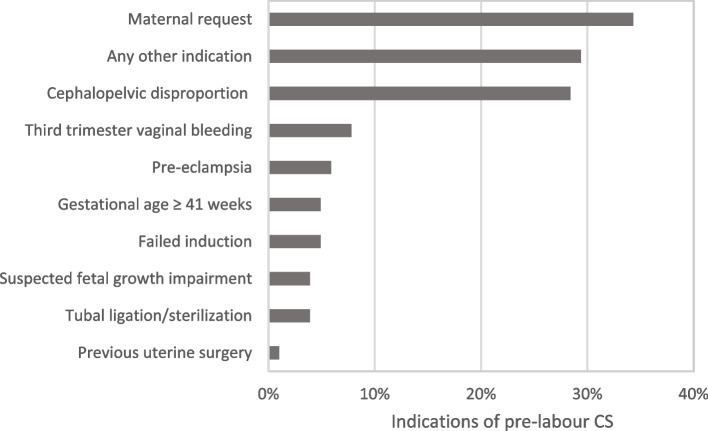
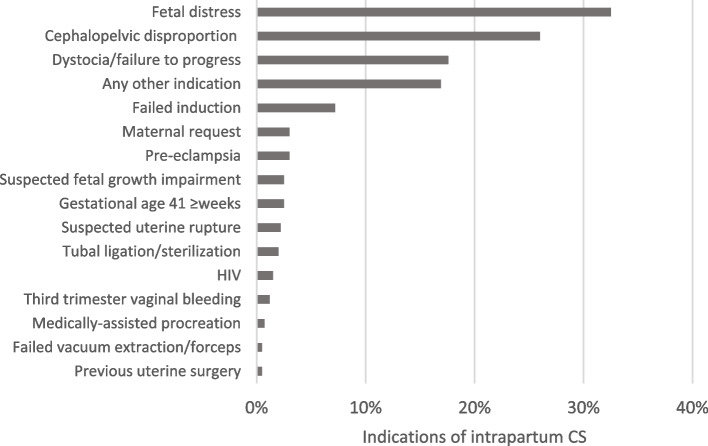
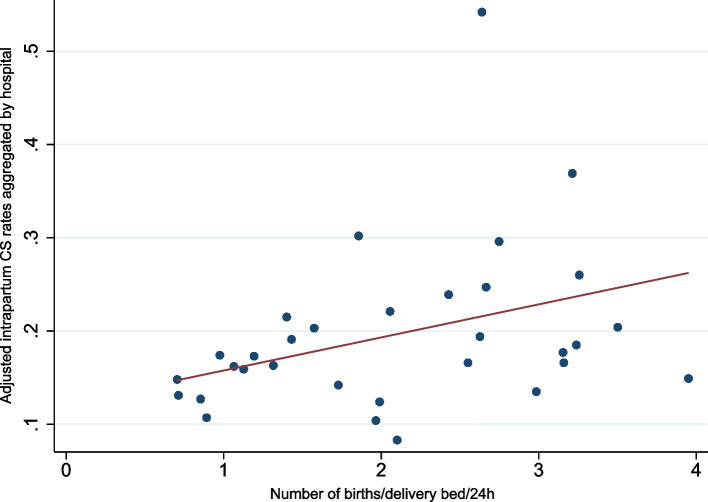
Results: A total of 2,092 low-risk women who had given birth in the participating hospitals were included. The overall CS rate was 24.1%, including 4.9% of pre-labour CS and 19.3% of intra-partum CS. Pre-labour CS was significantly associated with a 24-hour anaesthetist dedicated to the delivery ward (ORa = 3.70 [1.41; 9.72]) and with the possibility to have an individual room during labour and delivery (ORa = 0.28 [0.09; 0.87]). Intra-partum CS was significantly associated with a higher bed occupancy level (ORa = 1.45 [1.09; 1.93]): intrapartum CS rate would increase of 6.3% points if the average number of births per delivery bed per day increased by 10%.
Conclusion: Our results suggest that organisational norms and convenience associated with inadequate use of favourable resources, as well as the lack of privacy favouring women's preference for CS, and the excessive workload of healthcare providers drive the CS overuse in these hospitals. It is also crucial to enhance human and physical resources in delivery rooms and the organisation of intrapartum care to improve the birth experience and the working environment for those providing care.
Trial registration: The QUALI-DEC trial is registered on the Current Controlled Trials website ( https://www.isrctn.com/ ) under the number ISRCTN67214403.
Keywords: Caesarean section; Hospital organization; Low- and middle-income countries; Mode of birth.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Women's caesarean section preferences: A multicountry cross-sectional survey in low- and middle-income countries.Midwifery. 2024 May;132:103979. doi: 10.1016/j.midw.2024.103979. Epub 2024 Mar 22. Midwifery. 2024. PMID: 38520954
-
Implementing the QUALI-DEC project in Argentina, Burkina Faso, Thailand and Viet Nam: a process delineation and theory-driven process evaluation protocol.Glob Health Action. 2023 Dec 31;16(1):2290636. doi: 10.1080/16549716.2023.2290636. Epub 2023 Dec 22. Glob Health Action. 2023. PMID: 38133667 Free PMC article.
-
Implementation and evaluation of nonclinical interventions for appropriate use of cesarean section in low- and middle-income countries: protocol for a multisite hybrid effectiveness-implementation type III trial.Implement Sci. 2020 Sep 4;15(1):72. doi: 10.1186/s13012-020-01029-4. Implement Sci. 2020. PMID: 32887669 Free PMC article.
-
Continuous support for women during childbirth.Cochrane Database Syst Rev. 2017 Jul 6;7(7):CD003766. doi: 10.1002/14651858.CD003766.pub6. Cochrane Database Syst Rev. 2017. PMID: 28681500 Free PMC article.
-
Prevalence of and reasons for women's, family members', and health professionals' preferences for cesarean section in China: A mixed-methods systematic review.PLoS Med. 2018 Oct 16;15(10):e1002672. doi: 10.1371/journal.pmed.1002672. eCollection 2018 Oct. PLoS Med. 2018. PMID: 30325928 Free PMC article.
References
-
- Betrán AP, Ye J, Moller AB, Zhang J, Gülmezoglu AM, Torloni MR. The increasing trend in caesarean section rates: global, regional and national estimates: 1990–2014. PLoS One. 2016;11(2). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4743929/. Cited 2021 Jun 3. - PMC - PubMed
-
- Department of Reproductive Health and Research, World Health Organization. WHO statement on caesarean section rates. 2015. Available from: http://apps.who.int/iris/bitstream/handle/10665/161442/WHO_RHR_15.02_eng.... Cited 2021 Nov 23. - PubMed
-
- Vogel JP, Betrán AP, Vindevoghel N, Souza JP, Torloni MR, Zhang J, et al. Use of the Robson classification to assess caesarean section trends in 21 countries: a secondary analysis of two WHO multicountry surveys. Lancet Glob Health. 2015;3(5):e260–270. doi: 10.1016/S2214-109X(15)70094-X. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
