

Efficacy and safety of anti-PD-1 inhibitor versus anti-PD-L1 inhibitor in first-line treatment of extensive-stage small cell lung cancer: a multicenter retrospective study
- PMID: 38233798
- PMCID: PMC10795417
- DOI: 10.1186/s12885-024-11833-6
Efficacy and safety of anti-PD-1 inhibitor versus anti-PD-L1 inhibitor in first-line treatment of extensive-stage small cell lung cancer: a multicenter retrospective study
Abstract
Background: Immunotherapy targeting PD-1/PD-L1 has revolutionized the treatment of extensive-stage small cell lung cancer (ES-SCLC). However, clinical trials suggest differential efficacy of anti-PD-1 agents and anti-PD-L1 agents in first-line treatment of ES-SCLC. This retrospective multicenter study aimed to compare the efficacy and safety of anti-PD-1 agents versus anti-PD-L1 agents in first-line treatment of ES-SCLC in real-world practice.
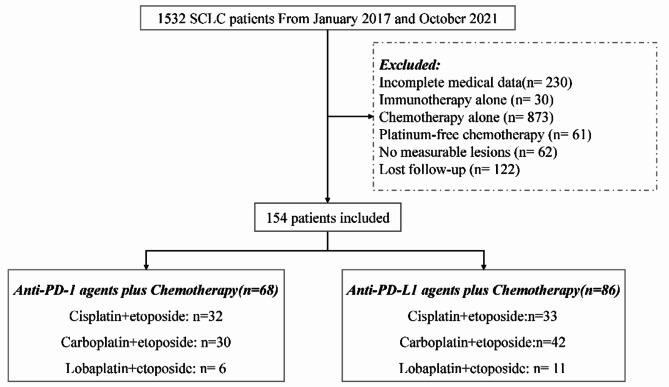
Methods: Patients with pathologically or cytologically confirmed ES-SCLC treated with platinum plus etoposide combined with anti-PD-1 or PD-L1 agents as first-line treatment in different centers of PLA General Hospital between January 2017 and October 2021 were included for this study. Survival outcomes and safety were compared between patients receiving anti-PD-1 and PD-L1 agents.
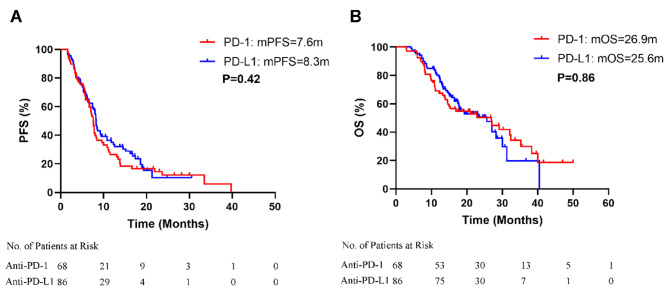
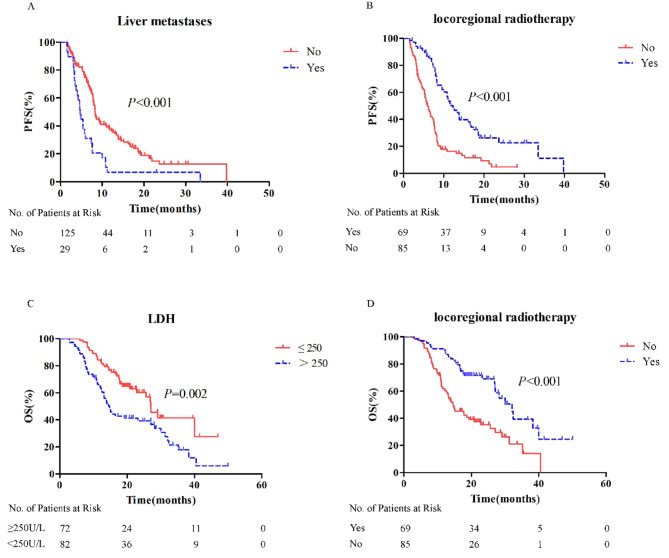
Results: Of the total 154 included patients, 68 received anti-PD-1 agents plus chemotherapy (PD-1 group), and 86 received anti-PD-L1 agents plus chemotherapy (PD-L1 group). Progression-free survival (PFS) and overall survival (OS) in the entire cohort were 7.6 months (95% confidence interval [CI]: 6.5-8.2 months) and 17.4 months (95% CI: 15.3-19.3 months), respectively. Median PFS and OS were comparable between the PD-1 group and PD-L1 group (PFS: 7.6 months vs. 8.3 months, HR = 1.13, 95% CI: 0.79-1.62, p = 0.415; OS: 26.9 months vs. 25.6 months, HR = 0.96, 95% CI: 0.63-1.47, p = 0.859. The objective response rate and disease control rate were comparable between the two groups: 79.4% vs. 79.1% and 92.6% vs. 94.2%, respectively. The 6-month, 12-month, and 18-month PFS and OS rates were slightly higher in the PD-L1 group than in the PD-1 group, while the 24-month PFS rate was slightly higher in the PD-1 group than in the PD-L1 group. Stratified analysis showed that locoregional thoracic radiotherapy and normal lactate dehydrogenase level were independent predictors of better OS in ES-SCLC patients treated with first-line chemotherapy plus ICI. Adverse events were not significantly different between the two groups.
Conclusions: Anti-PD-1 agents and anti-PD-L1 agents combined with chemotherapy as first-line treatment for ES-SCLC are comparably effective and well tolerated.
Keywords: Anti-PD-1/PD-L1; Immunotherapy; Lactate dehydrogenase; Locoregional thoracic radiotherapy; Small cell lung cancer.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Comparison of efficacy and safety between PD-1 inhibitors and PD-L1 inhibitors plus platinum-etoposide as first-line treatment for extensive-stage small-cell lung cancer: a multicenter, real-world analysis.BMC Cancer. 2023 Dec 6;23(1):1196. doi: 10.1186/s12885-023-11709-1. BMC Cancer. 2023. PMID: 38057736 Free PMC article.
-
Efficacy and safety of PD-1/PD-L1 inhibitor plus chemotherapy versus chemotherapy alone as first-line treatment for extensive-stage small cell lung cancer: A systematic review and meta-analysis.Thorac Cancer. 2020 Dec;11(12):3536-3546. doi: 10.1111/1759-7714.13698. Epub 2020 Oct 15. Thorac Cancer. 2020. PMID: 33058504 Free PMC article.
-
Efficacy and safety of PD-L1 inhibitors versus PD-1 inhibitors in first-line treatment with chemotherapy for extensive-stage small-cell lung cancer.Cancer Immunol Immunother. 2022 Mar;71(3):637-644. doi: 10.1007/s00262-021-03017-z. Epub 2021 Jul 23. Cancer Immunol Immunother. 2022. PMID: 34297160 Free PMC article.
-
Addition of thoracic radiotherapy to a PD-L1 inhibitor plus chemotherapy regimen delays brain metastasis onset in extensive-stage small cell lung cancer patients without baseline brain metastasis.Respir Res. 2025 Mar 5;26(1):85. doi: 10.1186/s12931-025-03157-1. Respir Res. 2025. PMID: 40045282 Free PMC article.
-
Combining PD-1 or PD-L1 inhibitors with chemotherapy is a good strategy for the treatment of extensive small cell lung cancer: A retrospective analysis of clinical studies.Front Immunol. 2022 Dec 5;13:1059557. doi: 10.3389/fimmu.2022.1059557. eCollection 2022. Front Immunol. 2022. PMID: 36544769 Free PMC article.
Cited by
-
Updated Bayesian network meta-analysis on the efficacy and safety of PD-1 versus PD-L1 inhibitors in first-line treatment with chemotherapy for extensive-stage small-cell lung cancer.Front Oncol. 2025 Jan 28;14:1455306. doi: 10.3389/fonc.2024.1455306. eCollection 2024. Front Oncol. 2025. PMID: 39935849 Free PMC article.
-
The Efficacy and Safety of Bevacizumab Plus Anti-PD-1/PD-L1 Inhibitors in Combination with Hepatic Arterial Infusion Chemotherapy for Initially Unresectable Hepatocellular Carcinoma.Immunotargets Ther. 2024 Oct 26;13:559-569. doi: 10.2147/ITT.S478685. eCollection 2024. Immunotargets Ther. 2024. PMID: 39478940 Free PMC article.
-
Enhancing cancer care with improved checkpoint inhibitors: a focus on PD-1/PD-L1.EXCLI J. 2024 Oct 29;23:1303-1326. doi: 10.17179/excli2024-7783. eCollection 2024. EXCLI J. 2024. PMID: 39624113 Free PMC article. Review.
-
Effectiveness and safety of anlotinib plus anti-programmed cell death 1/ligand 1 (anti-PD-1/PD-L1) antibodies as maintenance therapy after first-line chemotherapy combined with anti-PD-1/PD-L1 antibodies in extensive-stage small cell lung cancer: a real-world study.J Thorac Dis. 2024 Jul 30;16(7):4391-4399. doi: 10.21037/jtd-24-394. Epub 2024 Jul 5. J Thorac Dis. 2024. PMID: 39144292 Free PMC article.
-
Efficacy and safety of first-line chemoimmunotherapy in young patients with extensive-stage small cell lung cancer: a multicenter retrospective study.BMC Cancer. 2025 Jul 1;25(1):1136. doi: 10.1186/s12885-025-14524-y. BMC Cancer. 2025. PMID: 40597860 Free PMC article.
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA: a cancer journal for clinicians. 2022;72:7–33. 10.3322/caac.21708 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
