

Metabolic and other morbid complications in congenital generalized lipodystrophy type 4
- PMID: 38234231
- PMCID: PMC11060913
- DOI: 10.1002/ajmg.a.63533
Metabolic and other morbid complications in congenital generalized lipodystrophy type 4
Abstract
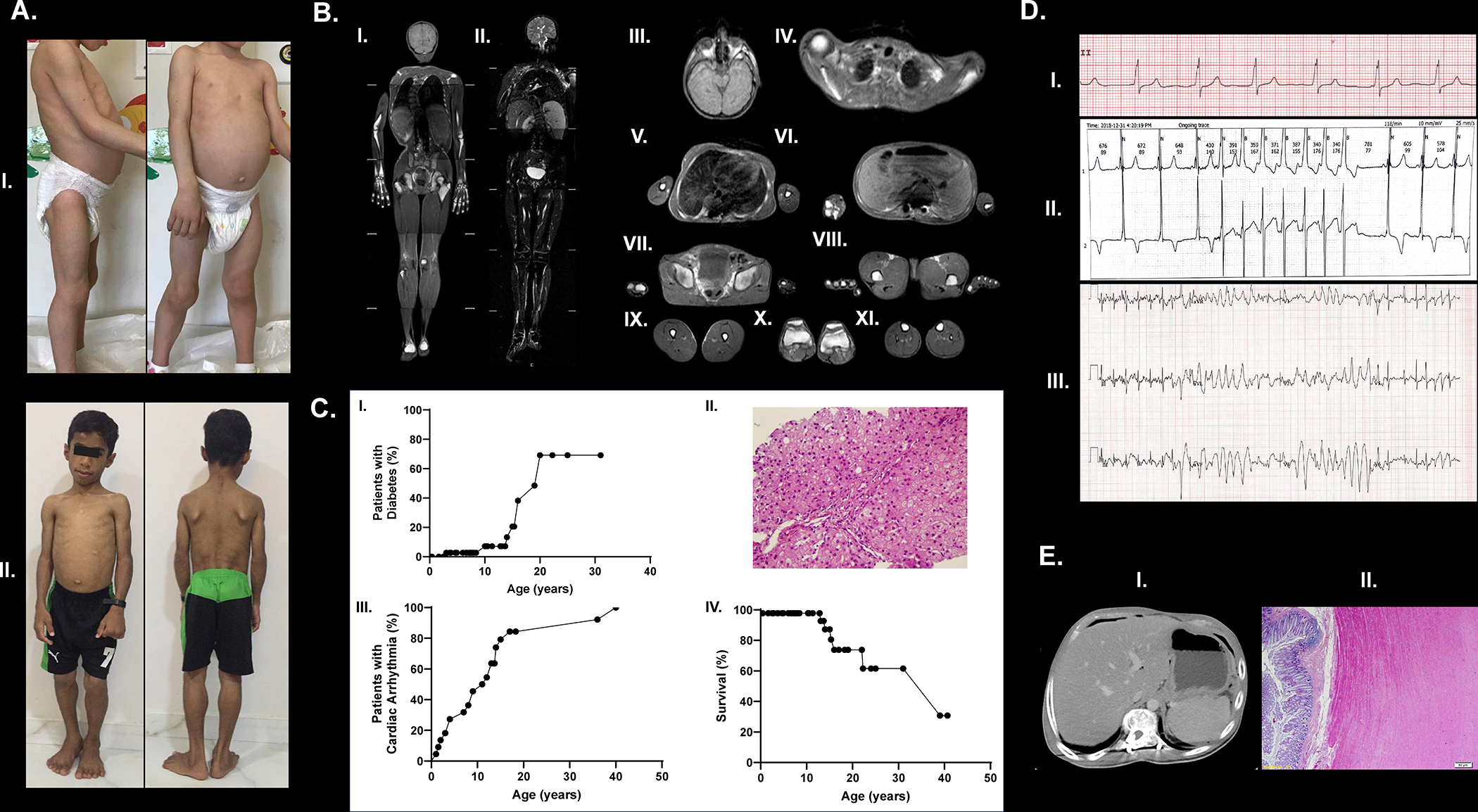
Morbidity and mortality rates in patients with autosomal recessive, congenital generalized lipodystrophy type 4 (CGL4), an ultra-rare disorder, remain unclear. We report on 30 females and 16 males from 10 countries with biallelic null variants in CAVIN1 gene (mean age, 12 years; range, 2 months to 41 years). Hypertriglyceridemia was seen in 79% (34/43), hepatic steatosis in 82% (27/33) but diabetes mellitus in only 21% (8/44). Myopathy with elevated serum creatine kinase levels (346-3325 IU/L) affected all of them (38/38). 39% had scoliosis (10/26) and 57% had atlantoaxial instability (8/14). Cardiac arrhythmias were detected in 57% (20/35) and 46% had ventricular tachycardia (16/35). Congenital pyloric stenosis was diagnosed in 39% (18/46), 9 had esophageal dysmotility and 19 had intestinal dysmotility. Four patients suffered from intestinal perforations. Seven patients died at mean age of 17 years (range: 2 months to 39 years). The cause of death in four patients was cardiac arrhythmia and sudden death, while others died of prematurity, gastrointestinal perforation, and infected foot ulcers leading to sepsis. Our study highlights high prevalence of myopathy, metabolic abnormalities, cardiac, and gastrointestinal problems in patients with CGL4. CGL4 patients are at high risk of early death mainly caused by cardiac arrhythmias.
Keywords: CAVIN1; congenital generalized lipodystrophy; gastrointestinal disease; metabolic abnormalities; myopathy; ventricular tachycardia.
© 2024 Wiley Periodicals LLC.
Conflict of interest statement
Conflict of interest
BA run projects for and/or served as a consultant, board member, steering committee member, and/or speaker to Alnylam, Amryt, Regeneron, ThirdRock Ventures, Astra Zeneca, Novonordisk, Boehringer Ingelheim, Sanofi, Bilim Ilac, ARIS, and Servier. AG consults for Amryt Pharma plc, Regeneron, Kyttaro Limited, Third Rock Ventures, and has received grant support from Amryt Pharma plc, Regeneron, Quintiles, Akcea Pharmaceuticals, and Intercept Pharmaceuticals. AG is a co-holder of patents for use of leptin for treating human lipoatrophy and method of determining predisposition to said treatment but receives no financial benefit. RJB reports research support from Amryt Pharmaceuticals and Regeneron Pharmaceuticals. EAO reports the following conflicts: Grant support: Aegerion Pharmaceuticals (now Amryt Pharmaceuticals), Ionis Pharmaceuticals, Akcea Therapeutics, Gemphire Therapeutics, GI Dynamics (current), AstraZeneca (past two years). Consultant or Advisor: AstraZeneca, Thera Therapeutics, and BMS (past), Aegerion Pharmaceuticals (now Amryt Pharmaceuticals), Regeneron Pharmaceuticals (current). Drug support: Aegerion Pharmaceuticals (now Amryt Pharmaceuticals), Akcea Therapeutics, Rhythm Pharmaceuticals (all current). Other support: Aegerion Pharmaceuticals (now Amryt Pharmaceuticals), Regeneron Pharmaceuticals (current). TS consulted for Amryt and received grant support for an investigator-initiated trial from Aegerion Pharmaceuticals (now Amryt Pharmaceuticals). MB received an Honorarium as a speaker for Amryt Pharmaceuticals. CK received fees for Lecture and Advisory Board Membership from Amryt Pharmaceuticals. MW has served as consultant for Alnylam, Amryt, LG Chem, Regeneron, ThirdRock Ventures and is PI in clinical studies sponsored by Amryt. NP served as board member and consultant for Amryt Pharmaceutical and Ionis. ES attended advisory board/steering committee meetings organized by Amryt Pharmaceuticals and Regeneron Pharmaceuticals, Inc. Other authors report no conflicts of interest.
Figures

References
-
- Adiyaman SC, J VS, De Laffolie J, Hahn A, Siebert R, Wabitsch M, & Kamrath C (2022). Congenital generalized lipodystrophy type 4 due to a novel PTRF/CAVIN1 pathogenic variant in a child: effects of metreleptin substitution. J Pediatr Endocrinol Metab, 35(7), 946–952. 10.1515/jpem-2022-0022 - DOI - PubMed
-
- Akinci B, Sahinoz M, & Oral E (2000). Lipodystrophy Syndromes: Presentation and Treatment. In Feingold KR, Anawalt B, Boyce A, Chrousos G, de Herder WW, Dhatariya K, Dungan K, Hershman JM, Hofland J, Kalra S, Kaltsas G, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrere B, Levy M, McGee EA, McLachlan R, Morley JE, New M, Purnell J, Sahay R, Singer F, Sperling MA, Stratakis CA, Trence DL, & Wilson DP (Eds.), Endotext. https://www.ncbi.nlm.nih.gov/pubmed/29989768 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
