

Expert management of congenital portosystemic shunts and their complications
- PMID: 38234409
- PMCID: PMC10792643
- DOI: 10.1016/j.jhepr.2023.100933
Expert management of congenital portosystemic shunts and their complications
Erratum in
-
Corrigendum to "Expert management of congenital portosystemic shunts and their complications" [JHEP Reports 6 (2024)].JHEP Rep. 2024 Jan 30;6(3):101024. doi: 10.1016/j.jhepr.2024.101024. eCollection 2024 Mar. JHEP Rep. 2024. PMID: 38481635 Free PMC article.
Abstract
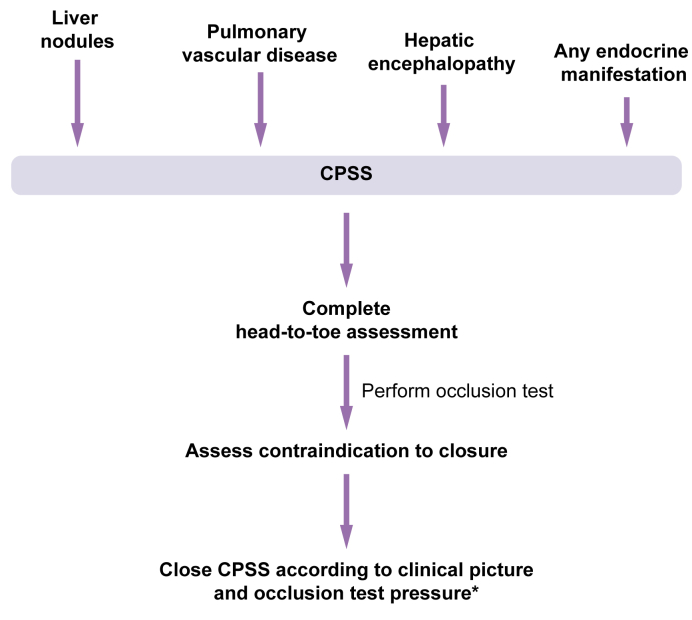
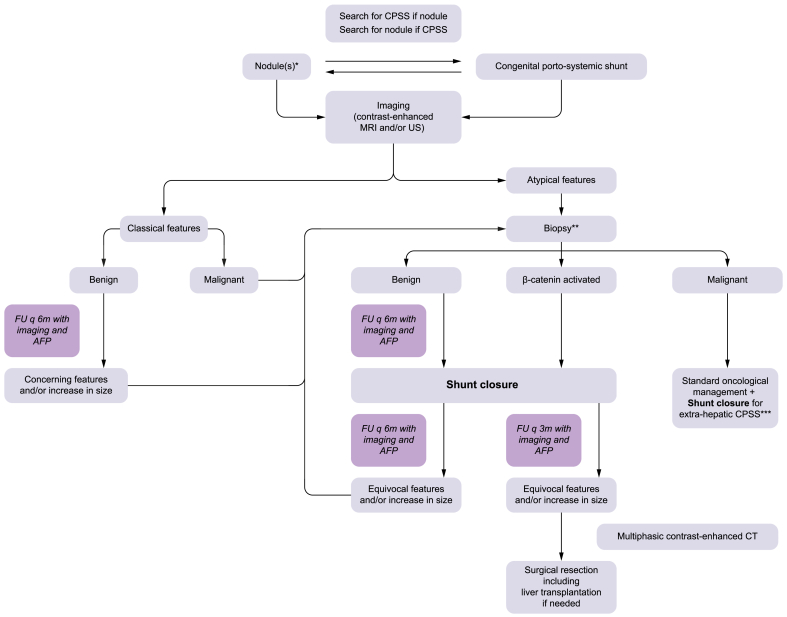
Congenital portosystemic shunts are often associated with systemic complications, the most challenging of which are liver nodules, pulmonary hypertension, endocrine abnormalities, and neurocognitive dysfunction. In the present paper, we offer expert clinical guidance on the management of liver nodules, pulmonary hypertension, and endocrine abnormalities, and we make recommendations regarding shunt closure and follow-up.
Keywords: adenoma; congenital portosystemic shunt; focal nodular hyperplasia; hepatocellular carcinoma; hyperandrogenism; hyperinsulinism; hypoglycemia; occlusion test; portal pressure; puberty; pulmonary hypertension; β-catenin.
© 2023 The Author(s).
Conflict of interest statement
The authors declare no conflicts of interest that pertain to this work. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources
