

Successful repair of an encephalocele wound in a child following a car accident: A case report
- PMID: 38234611
- PMCID: PMC10790164
- DOI: 10.3892/etm.2023.12339
Successful repair of an encephalocele wound in a child following a car accident: A case report
Abstract
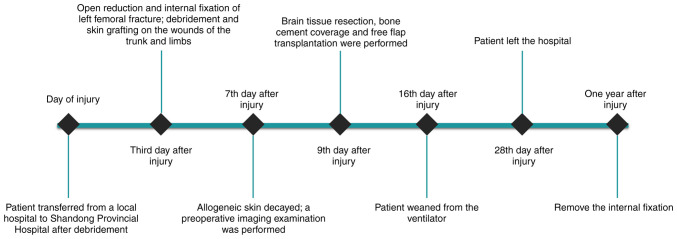
Repair of large cranial complex traumas in children is difficult. Notably, children have poorer underlying conditions than adults and are frailer under trauma. In addition, children have more limited treatment options, leading to the need to consider long-term functional and aesthetic outcomes. The present report describes the case of a 2-year-old child weighing 9 kg who experienced a skull fracture with encephalocele after a car accident and had a poor underlying condition. An artificial dura mater combined with bone cement was used to repair the skull, and then a free latissimus dorsi muscle flap (LDMF) combined with a split-thickness skin graft (STSG) was used to cover the wound, allowing the child to overcome the life-threatening situation as soon as possible with a satisfactory outcome. LDMF combined with STSG is an ideal option in repairing head wounds in children. Preoperative imaging and postoperative care also serve an important role in the success of the operation. When the situation is critical, multidisciplinary team treatment can guarantee the safety of the child.
Keywords: LDMF; STSG; encephalocele; scalp reconstruction; trauma.
Copyright © 2023, Spandidos Publications.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
[Application of computed tomographic angiography in repairing skin defect after scalp avulsion with free latissimus dorsi flap transplantation].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013 Mar;27(3):299-303. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013. PMID: 23672129 Chinese.
-
Free latissimus dorsi flap transfer for subtotal scalp and cranium defect reconstruction: report of 7 cases.Microsurgery. 2007;27(5):425-8. doi: 10.1002/micr.20386. Microsurgery. 2007. PMID: 17596862
-
A Standard Algorithm for Reconstruction of Scalp Defects With Simultaneous Free Flaps in an Interdisciplinary Two-Team Approach.Front Oncol. 2019 Oct 25;9:1130. doi: 10.3389/fonc.2019.01130. eCollection 2019. Front Oncol. 2019. PMID: 31709189 Free PMC article.
-
[Recurring post-traumatic growing skull fracture].Rev Neurol. 2015 Apr 16;60(8):351-4. Rev Neurol. 2015. PMID: 25857859 Review. Spanish.
-
Indications and outcomes of free tissue transfer to the lower extremity in children: review.J Reconstr Microsurg. 2006 Apr;22(3):173-81. doi: 10.1055/s-2006-939963. J Reconstr Microsurg. 2006. PMID: 16780046 Review.
References
-
- Xi C, Yao H, Xu Y, Liu Y, Tian H, Hu J. The emergency epidemiologic characteristics of casualties cases with head injury in Shanghai. Chin J Emerg Med. 2008;17:1131–1134.
Publication types
LinkOut - more resources
Full Text Sources