

Adenosine Receptor Subtypes and Cardioprotection
- PMID: 38234711
- PMCID: PMC10792443
- DOI: 10.1002/(sici)1098-2299(199811/12)45:3/4<394::aid-ddr40>3.0.co;2-j
Adenosine Receptor Subtypes and Cardioprotection
Abstract
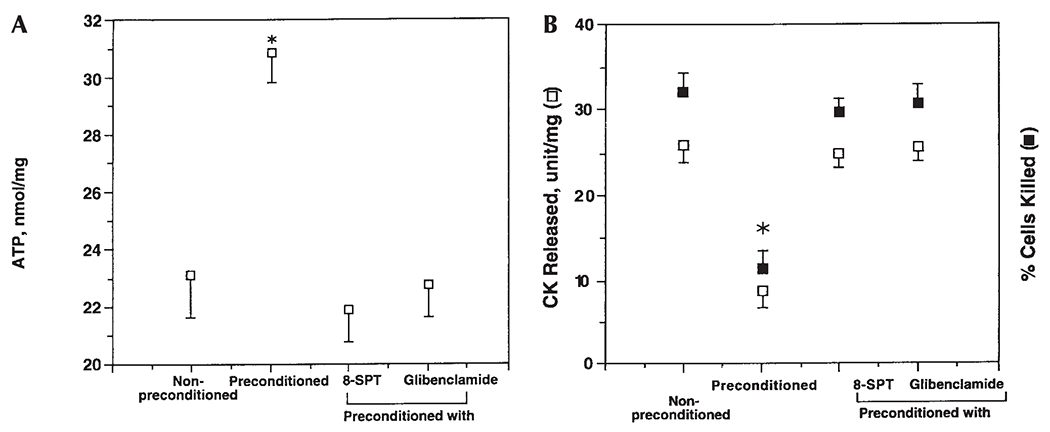
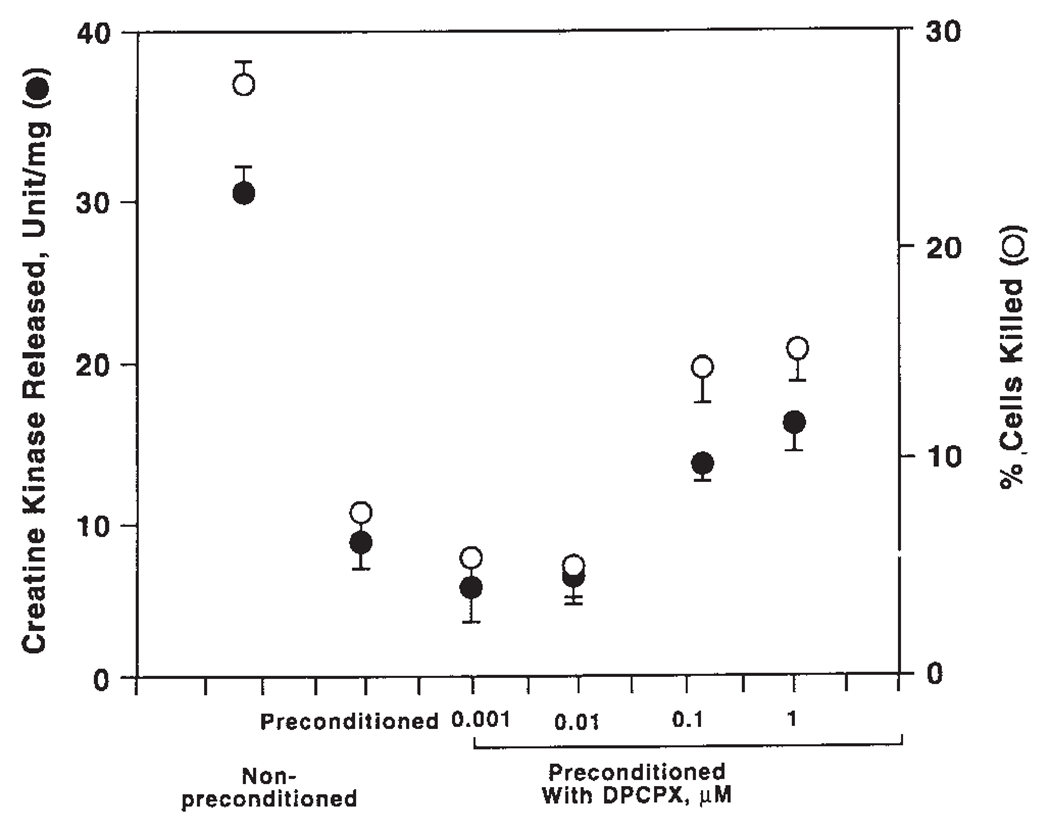
Brief ischemia prior to a sustained period of ischemia reduces myocardial infarct size, a phenomenon known as preconditioning. A cardiac ventricular myocyte model has been developed to investigate the role and signaling mechanism of adenosine receptor subtypes in cardiac preconditioning. A 5-min exposure of cardiac myocytes to simulated ischemia, termed preconditioning ischemia, prior to a subsequent 90-min period of ischemia protected them against injury incurred during the 90-min ischemia. Preconditioning ischemia preserved ATP content, reduced percentage of cells killed, and decreased release of creatine kinase into the medium. Activation of the adenosine A1 receptor with CCPA or the A3 receptor with IB-MECA can replace preconditioning ischemia and mimic the protective effect of preconditioning ischemia. Blockade of the A1 receptor with its selective antagonist DPCPX or of the A3 receptor with the A3 selective antagonist MRS1191 during the preconditioning ischemia resulted in only a partial attenuation of the subsequent protection. Incubation with both DPCPX and MRS1191 or with the nonselective antagonist 8-SPT during the preconditioning ischemia completely abolished the protective effect of preconditioning ischemia. The KATP channel opener pinacidil caused a large activation of the KATP channel current and was able to precondition the myocyte. The KATP channel antagonist glibenclamide blocked the cardioprotective effect of preconditioning ischemia when it was included during myocyte exposure to the preconditioning ischemia, indicating that KATP channel is a requisite effector in mediating preconditioning. A receptor-mediated stimulation of phospholipase C or phospholipase D, with consequent activation of protein kinase C and KATP channel, appears to be the signaling mechanism linking adenosine A1 and A3 receptors to the induction of preconditioning. A model of how ischemic preconditioning is triggered and mediated is proposed. Evidence is accumulating to support its validity.
Keywords: adenosine; ischemia; myocardium; purinergic; receptor.
Figures




Similar articles
-
Direct preconditioning of cardiac ventricular myocytes via adenosine A1 receptor and KATP channel.Am J Physiol. 1996 Nov;271(5 Pt 2):H1769-77. doi: 10.1152/ajpheart.1996.271.5.H1769. Am J Physiol. 1996. PMID: 8945890
-
Protein kinase C-dependent activation of KATP channel enhances adenosine-induced cardioprotection.Biochem J. 1998 Dec 1;336 ( Pt 2)(Pt 2):337-43. doi: 10.1042/bj3360337. Biochem J. 1998. PMID: 9820809 Free PMC article.
-
Dual activation of adenosine A1 and A3 receptors mediates preconditioning of isolated cardiac myocytes.Eur J Pharmacol. 1997 Feb 12;320(2-3):241-8. doi: 10.1016/s0014-2999(96)00901-6. Eur J Pharmacol. 1997. PMID: 9059860
-
Adenosine and preconditioning revisited.Clin Exp Pharmacol Physiol. 1999 Feb;26(2):92-9. doi: 10.1046/j.1440-1681.1999.03003.x. Clin Exp Pharmacol Physiol. 1999. PMID: 10065327 Review.
-
[-Myocardial protection by preconditioning. Experimental and clinical significance-].Z Kardiol. 1996 Feb;85(2):79-89. Z Kardiol. 1996. PMID: 8650986 Review. German.
Cited by
-
Synthetic Small-Molecule Ligands Targeted to Adenosine Receptors: Is There Potential Towards Ischemic Heart Disease?Cells. 2025 Aug 7;14(15):1219. doi: 10.3390/cells14151219. Cells. 2025. PMID: 40801651 Free PMC article. Review.
References
-
- Armstrong S, Ganote CE. 1994. Adenosine receptor specificity in preconditioning of isolated rabbit cardiomyocytes: Evidence of A3 receptor involvement. Cardiovasc Res 28:1049–1056. - PubMed
-
- Auchampach JA, Grover GJ, Gross GJ. 1992. Blockade of ischemic preconditioning in dogs by the novel ATP dependent potassium channel antagonist sodium 5-hydroxydecanoate. Cardiovas Res 26:1054–1062. - PubMed
-
- Babbitt DG, Virmani R, Forman MB. 1989. Intracoronary adenosine administered after reperfusion limits vascular injury after prolonged ischemia in the canine model. Circulation 80:1388–1399. - PubMed
-
- Cribier AL, Korsatz R, Koning P Rath H, Gamra H, Stix G, Merchant S, Chan C, Letac B. 1992. Improved myocardial ischemic response and enhanced collateral circulation with long repetitive coronary occlusion during angioplasty: A prospective study. J Am Coll Cariol 20:578–586. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
