

Streptococcus intermedius: From a Normal Oral Commensal to a Life-Threatening Organism
- PMID: 38234954
- PMCID: PMC10792467
- DOI: 10.7759/cureus.50708
Streptococcus intermedius: From a Normal Oral Commensal to a Life-Threatening Organism
Abstract
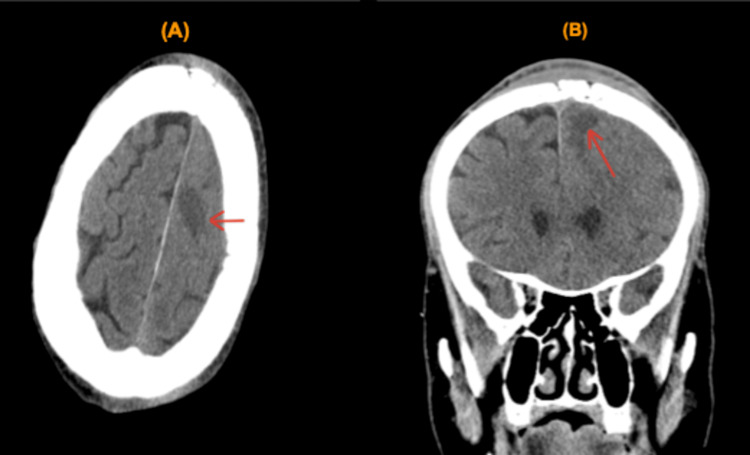
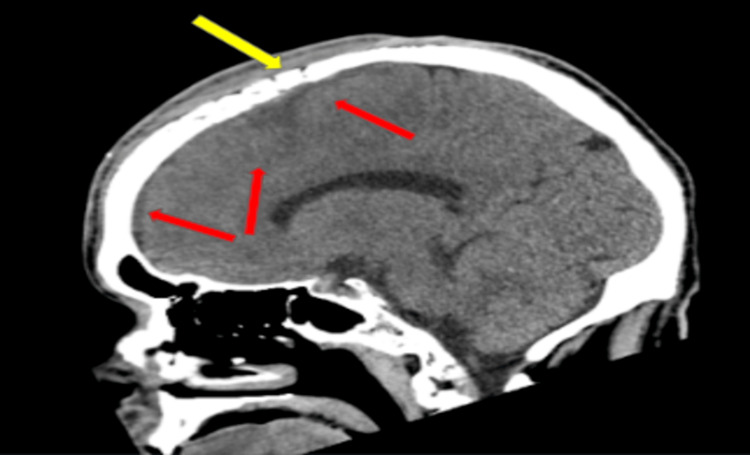
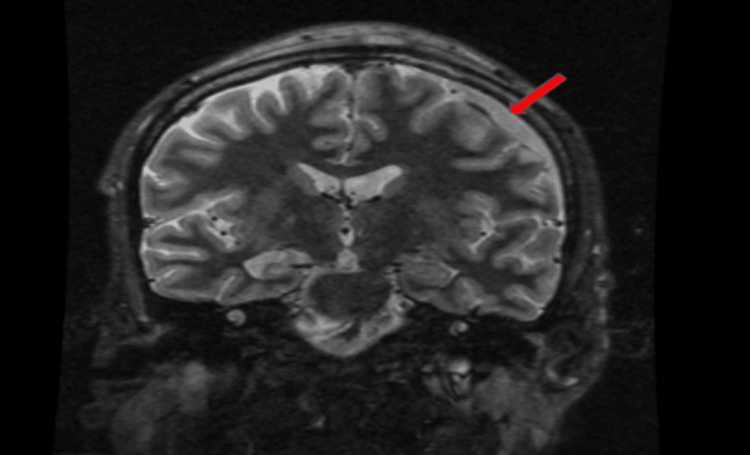
Subdural empyema is a collection of pus in the subdural space between the dura mater and the arachnoid. It carries very high morbidity and mortality as it can spread anywhere in the brain; however, the risk can be mitigated with appropriate surgical and medical intervention. Being protected by the skull, cranial infections are usually preceded by a significant risk factor, either an external invader such as skull fractures secondary to trauma, penetrating injury, prior surgery, or, more commonly, in more than 50% of cases, due to spread of an internal infection such as ear or sinus infections. Anaerobic and aerobic bacteria can cause subdural empyema. Both gram-positive and gram-negative bacteria are notorious for developing this kind of infection; for example, different groups of gram-positive streptococci and staphylococci, gram-negative Haemophilus influenza, and other gram-negative bacilli can cause subdural empyema. While streptococci are more frequent with sinus infection causing subdural empyema, staphylococci are associated with skin invasion secondary to either head trauma or cranial surgery. Streptococcus intermedius is a gram-positive alpha-hemolytic pathogen belonging to the larger Streptococcus anginosus group that itself is a subgroup from viridans streptococci, aka Streptococcus milleri. Streptococcus intermedius is an oral commensal flora and is considered to be a low-virulence bacteria in immunocompetent patients but can be associated with significant morbidity and mortality. Subdural empyema tends to occur more often in immunocompromised patients such as diabetic patients, those with human immunodeficiency virus infection, and those using immunosuppressive medications. The clinical course ranges from indolent to fulminant. The size and location of the abscess play a role in clinical presentation. Headache is the most common presenting symptom, but patients can also present with fever, nausea, seizure, or altered mental status. Diagnosis can be obtained with CT and MRI scans of the brain. Prompt drainage of the abscess and lengthy antibiotics improve the prognosis significantly. Our case highlights a rare origin of subdural empyema from the direct spread of a skin abscess.
Keywords: brain abscess; craniotomy; diabetes mellitus; emergency medicine; medical intensive care unit (micu); neurosurgery; seizure; skin abscess; streptococcus intermedius bacteremia; subdural empyema.
Copyright © 2023, Mahmoud et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Subdural empyema and cranial epidural abscess. Silverberg AL, DiNubile MJ. Med Clin North Am. 1985;69:361–374. - PubMed
-
- Subdural empyema in children--20-year experience in a medical center. Wu TJ, Chiu NC, Huang FY. https://pubmed.ncbi.nlm.nih.gov/18327428/ J Microbiol Immunol Infect. 2008;41:62–67. - PubMed
-
- Bacterial infections of the central nervous system. Suthar R, Sankhyan N. Indian J Pediatr. 2019;86:60–69. - PubMed
-
- Subdural empyema of the cervical spine: clinicopathological correlates and magnetic resonance imaging. Report of three cases. Levy ML, Wieder BH, Schneider J, Zee CS, Weiss MH. J Neurosurg. 1993;79:929–935. - PubMed
-
- Subdural empyema. Greenlee JE. Curr Treat Options Neurol. 2003;5:13–22. - PubMed
Publication types
LinkOut - more resources
Full Text Sources