

Facts and Hopes in Using Omics to Advance Combined Immunotherapy Strategies
- PMID: 38236069
- PMCID: PMC11062841
- DOI: 10.1158/1078-0432.CCR-22-2241
Facts and Hopes in Using Omics to Advance Combined Immunotherapy Strategies
Abstract
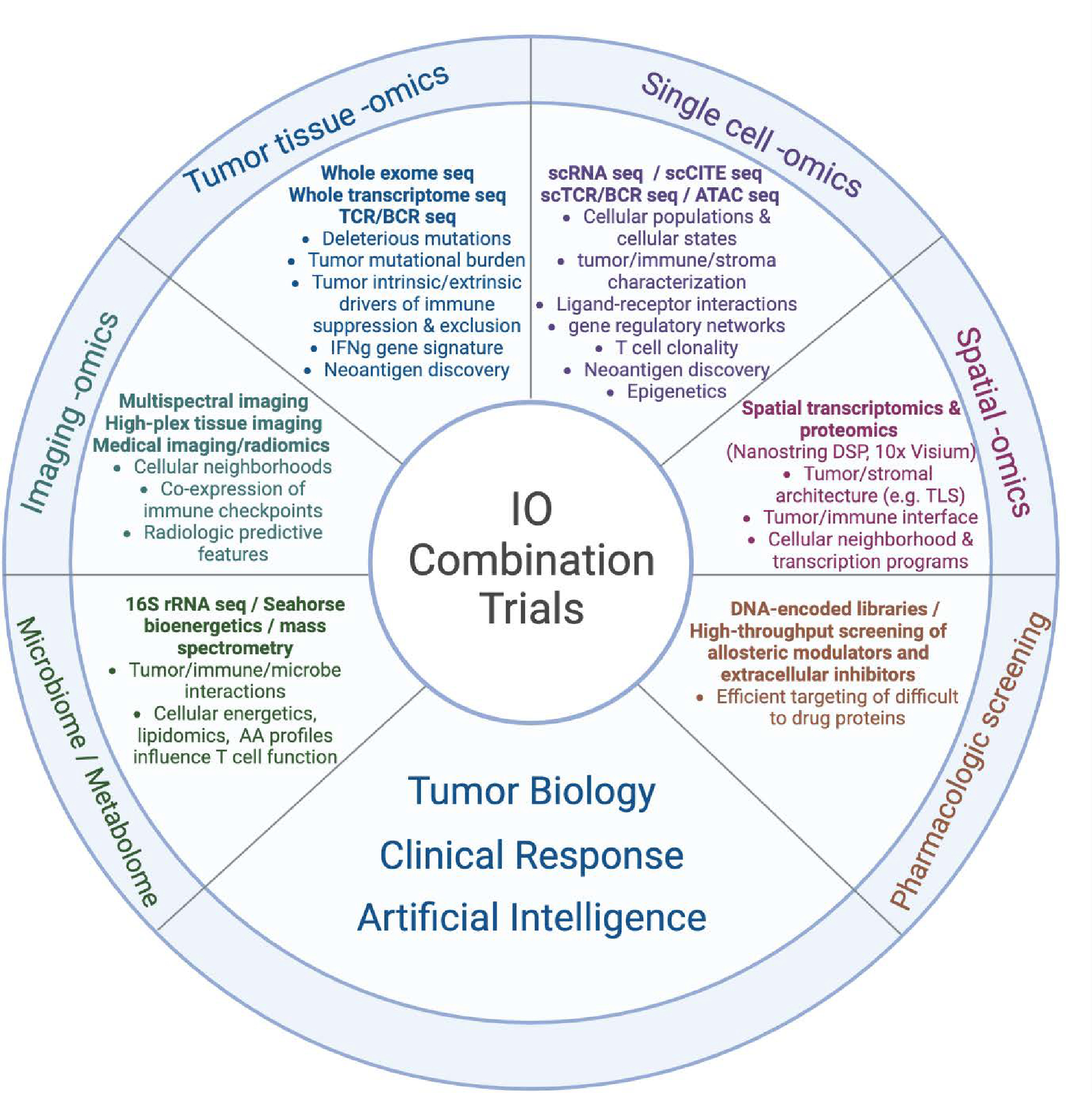
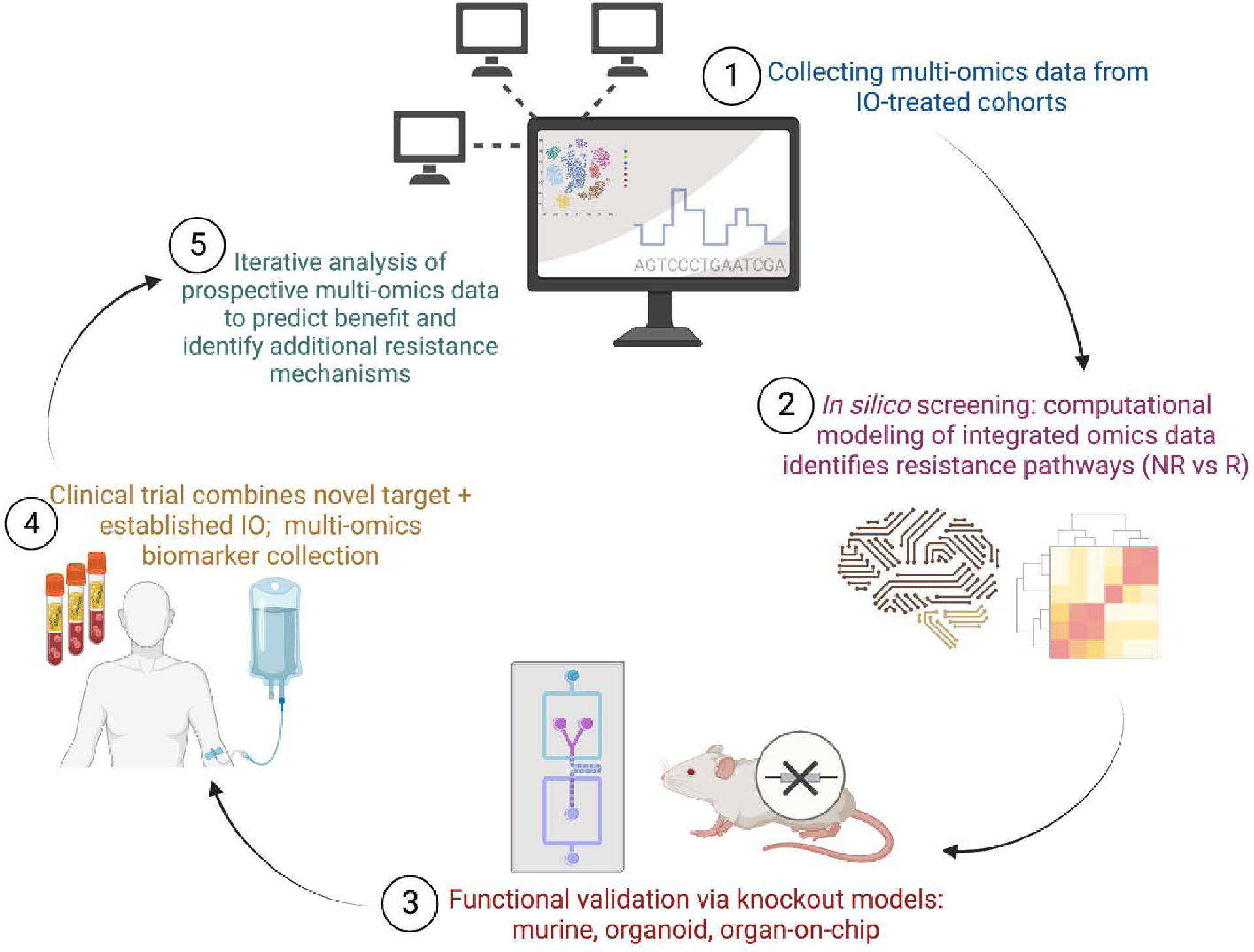
The field of oncology has been transformed by immune checkpoint inhibitors (ICI) and other immune-based agents; however, many patients do not receive a durable benefit. While biomarker assessments from pivotal ICI trials have uncovered certain mechanisms of resistance, results thus far have only scraped the surface. Mechanisms of resistance are as complex as the tumor microenvironment (TME) itself, and the development of effective therapeutic strategies will only be possible by building accurate models of the tumor-immune interface. With advancement of multi-omic technologies, high-resolution characterization of the TME is now possible. In addition to sequencing of bulk tumor, single-cell transcriptomic, proteomic, and epigenomic data as well as T-cell receptor profiling can now be simultaneously measured and compared between responders and nonresponders to ICI. Spatial sequencing and imaging platforms have further expanded the dimensionality of existing technologies. Rapid advancements in computation and data sharing strategies enable development of biologically interpretable machine learning models to integrate data from high-resolution, multi-omic platforms. These models catalyze the identification of resistance mechanisms and predictors of benefit in ICI-treated patients, providing scientific foundation for novel clinical trials. Moving forward, we propose a framework by which in silico screening, functional validation, and clinical trial biomarker assessment can be used for the advancement of combined immunotherapy strategies.
©2024 American Association for Cancer Research.
Figures
References
-
- de Castro G, Kudaba I, Wu YL, Lopes G, Kowalski DM, Turna HZ, et al. Five-Year Outcomes With Pembrolizumab Versus Chemotherapy as First-Line Therapy in Patients With Non–Small-Cell Lung Cancer and Programmed Death Ligand-1 Tumor Proportion Score ≥ 1% in the KEYNOTE-042 Study. J Clin Oncol. 2022. Oct 28;JCO.21.02885. - PMC - PubMed
-
- Wolchok JD, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. CheckMate 067: 6.5-year outcomes in patients (pts) with advanced melanoma. J Clin Oncol. 2021. May 20;39(15_suppl):9506–9506.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
