

Pregnancy-associated changes in urinary uromodulin excretion in chronic hypertension
- PMID: 38236469
- PMCID: PMC11150301
- DOI: 10.1007/s40620-023-01830-6
Pregnancy-associated changes in urinary uromodulin excretion in chronic hypertension
Abstract
Background: Pregnancy involves major adaptations in renal haemodynamics, tubular, and endocrine functions. Hypertensive disorders of pregnancy are a leading cause of maternal mortality and morbidity. Uromodulin is a nephron-derived protein that is associated with hypertension and kidney diseases. Here we study the role of urinary uromodulin excretion in hypertensive pregnancy.
Methods: Urinary uromodulin was measured by ELISA in 146 pregnant women with treated chronic hypertension (n = 118) and controls (n = 28). We studied non-pregnant and pregnant Wistar Kyoto and Stroke Prone Spontaneously Hypertensive rats (n = 8/strain), among which a group of pregnant Stroke-Prone Spontaneously Hypertensive rats was treated with either nifedipine (n = 7) or propranolol (n = 8).
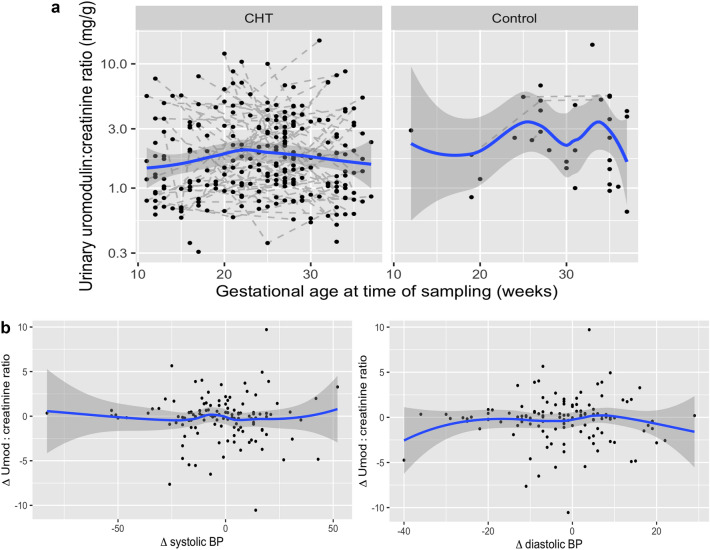
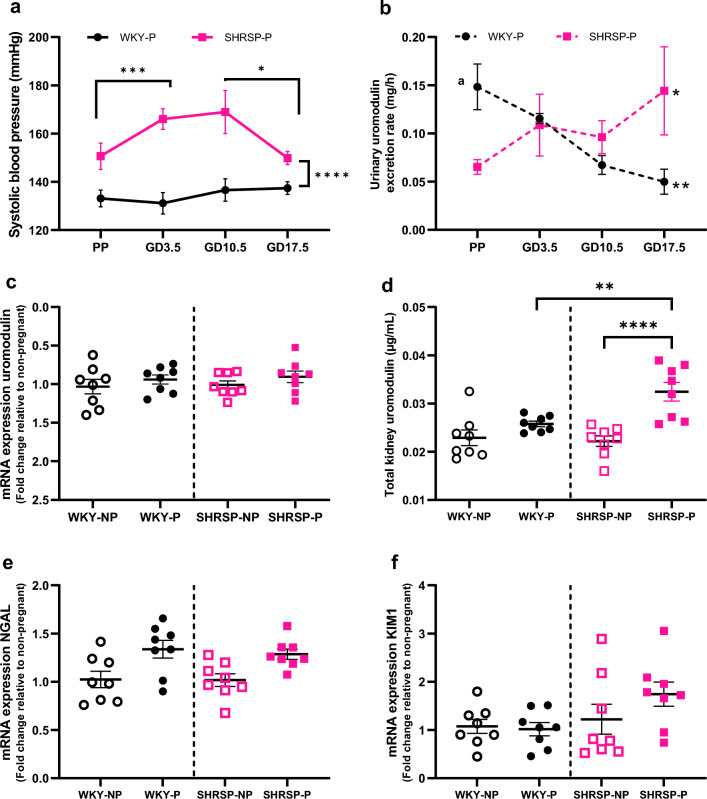
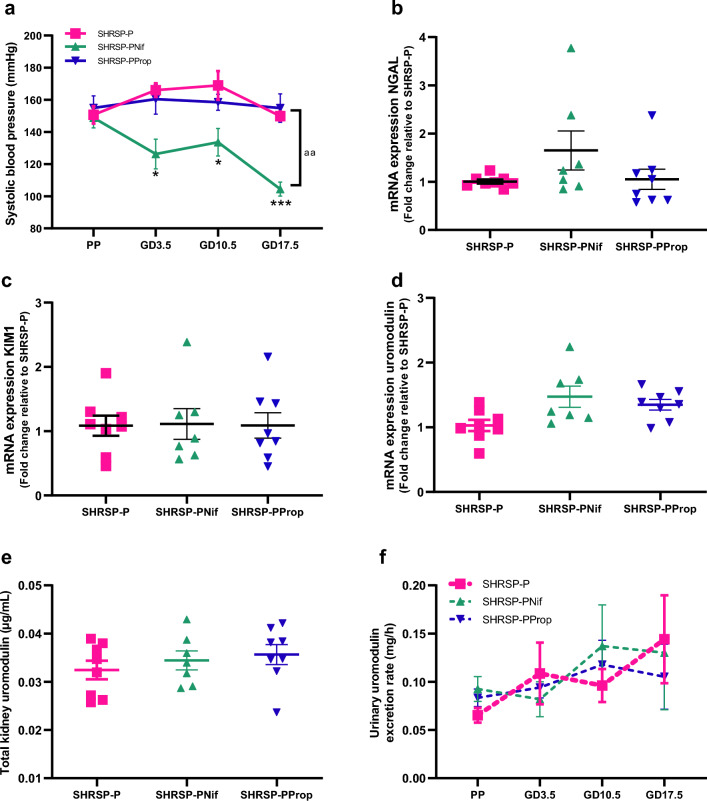
Results: In pregnant women, diagnosis of chronic hypertension, increased maternal body mass index, Black maternal ethnicity and elevated systolic blood pressure at the first antenatal visit were significantly associated with a lower urinary uromodulin-to-creatinine ratio. In rodents, pre-pregnancy urinary uromodulin excretion was twofold lower in Stroke-Prone Spontaneously Hypertensive rats than in Wistar Kyoto rats. During pregnancy, the urinary uromodulin excretion rate gradually decreased in Wistar Kyoto rats (a twofold decrease), whereas a 1.5-fold increase was observed in Stroke-Prone Spontaneously Hypertensive rats compared to pre-pregnancy levels. Changes in uromodulin were attributed by kidney injury in pregnant rats. Neither antihypertensive changed urinary uromodulin excretion rate in pregnant Stroke-Prone Spontaneously Hypertensive rats.
Conclusions: In summary, we demonstrate pregnancy-associated differences in urinary uromodulin: creatinine ratio and uromodulin excretion rate between chronic hypertensive and normotensive pregnancies. Further research is needed to fully understand uromodulin physiology in human pregnancy and establish uromodulin's potential as a biomarker for renal adaptation and renal function in pregnancy.
Keywords: Blood pressure; Chronic hypertensive pregnancy; Kidney physiology; Uromodulin.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
