

Outcomes after stenting of renal artery stenosis in patients with high-risk clinical features
- PMID: 38236490
- PMCID: PMC10796309
- DOI: 10.1186/s43044-024-00435-z
Outcomes after stenting of renal artery stenosis in patients with high-risk clinical features
Erratum in
-
Correction: Outcomes after stenting of renal artery stenosis in patients with high-risk clinical features.Egypt Heart J. 2024 Feb 1;76(1):15. doi: 10.1186/s43044-024-00445-x. Egypt Heart J. 2024. PMID: 38300423 Free PMC article. No abstract available.
Abstract
Background: In patients with renal artery stenosis, revascularization was seen as a mean to improve outcomes, but large studies failed to show significant benefit in general population. However, data on benefits of renal artery stenting in patients with high-risk features, such as rapidly declining renal function and cardiac destabilization syndromes, are limited, as they were excluded from trials. In this descriptive study, we aimed to evaluate short- and long-term outcomes in high-risk patients with renal artery stenosis, treated by angioplasty and stenting. We have retrospectively interrogated our local databases for renal artery percutaneous interventions; patients at high-risk (rapidly declining renal function; stable chronic renal failure and bilateral renal artery disease; severe hypertensive crisis) were selected for the current analysis.
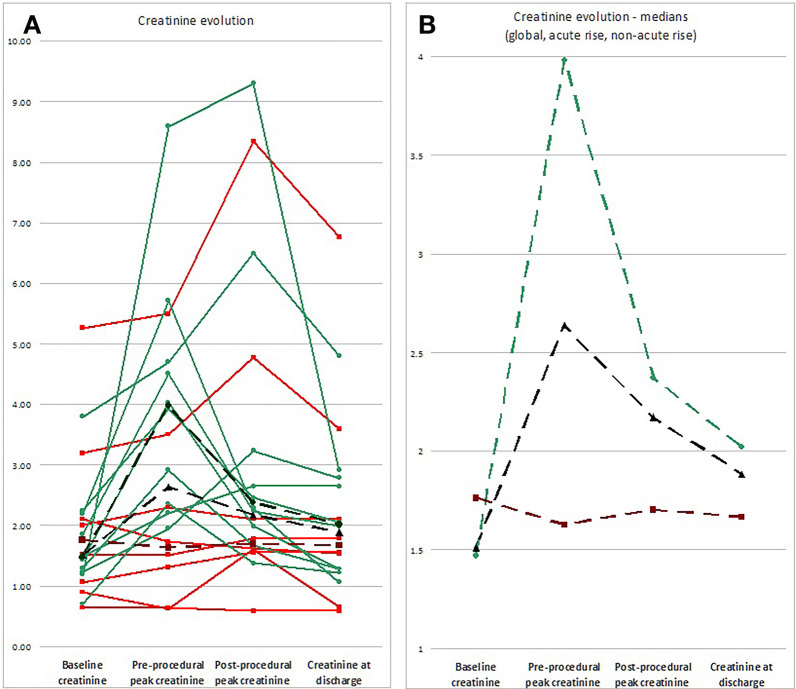
Results: Of 30 patients undergoing renal artery stenting, 18 patients were deemed "high-risk." On short term, good in-hospital control of hypertension and cardiac stabilization were obtained in all patients. Renal function improved significantly only in patients admitted with rapidly declining renal function, with significant creatinine level fall from median 3.98 mg/dL to 2.02 mg/dL, p = 0.023. However, for the whole group, creatinine change was non-significant (- 0.12 mg/dL, p = NS). On the long term, five patients (27.8%) ended-up on chronic hemodialysis and six patients died (33.3%) after a median of 20 months. No death occurred during the first year after the procedure.
Conclusions: Percutaneous procedures are feasible and safe in patients with high-risk renal artery stenosis, especially in those with rapidly declining renal function, probably saving some of them from the immediate need for renal replacement therapy, but long-term results are negatively influenced by the precarious general and cardio-vascular status of these patients and by the pre-existing significant renal parenchymal disease, non-related to the renal artery stenosis.
Keywords: Cardiac destabilization syndromes; Rapidly declining renal function; Renal artery disease; Renal artery stenting.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Stenting for peripheral artery disease of the lower extremities: an evidence-based analysis.Ont Health Technol Assess Ser. 2010;10(18):1-88. Epub 2010 Sep 1. Ont Health Technol Assess Ser. 2010. PMID: 23074395 Free PMC article.
-
Long-Term Mortality After Renal Artery Stenting in Patients With Severe Atherosclerotic Renal Artery Stenosis and High-Risk Clinical Manifestations.Am J Hypertens. 2021 Aug 9;34(8):880-887. doi: 10.1093/ajh/hpab027. Am J Hypertens. 2021. PMID: 33530094
-
[The long-term results percutaneous transluminal angioplasty and stenting in atherosclerotic renal artery stenosis].Zhonghua Nei Ke Za Zhi. 2006 Oct;45(10):804-6. Zhonghua Nei Ke Za Zhi. 2006. PMID: 17217742 Chinese.
-
Current Status of Renal Artery Angioplasty and Stenting for Resistant Hypertension: A Case Series and Review of the Literature.Curr Hypertens Rev. 2017;13(2):93-103. doi: 10.2174/1573402113666170804153026. Curr Hypertens Rev. 2017. PMID: 28782466 Review.
-
Issues related to renal artery angioplasty and stenting.Vascular. 2017 Dec;25(6):618-628. doi: 10.1177/1708538116677654. Epub 2017 Aug 7. Vascular. 2017. PMID: 28782453 Review.
Cited by
-
Correction: Outcomes after stenting of renal artery stenosis in patients with high-risk clinical features.Egypt Heart J. 2024 Feb 1;76(1):15. doi: 10.1186/s43044-024-00445-x. Egypt Heart J. 2024. PMID: 38300423 Free PMC article. No abstract available.
-
Gestational Hydronephrosis: A Retrospective Analysis of the Clinical Outcomes of Ureteral Stent Placement Versus Conservative Treatment.Medicina (Kaunas). 2025 May 4;61(5):845. doi: 10.3390/medicina61050845. Medicina (Kaunas). 2025. PMID: 40428803 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous