

Pre-hospital rule-out of non-ST-segment elevation acute coronary syndrome by a single troponin: final one-year outcomes of the ARTICA randomised trial
- PMID: 38236708
- PMCID: PMC11307197
- DOI: 10.1093/ehjqcco/qcae004
Pre-hospital rule-out of non-ST-segment elevation acute coronary syndrome by a single troponin: final one-year outcomes of the ARTICA randomised trial
Abstract
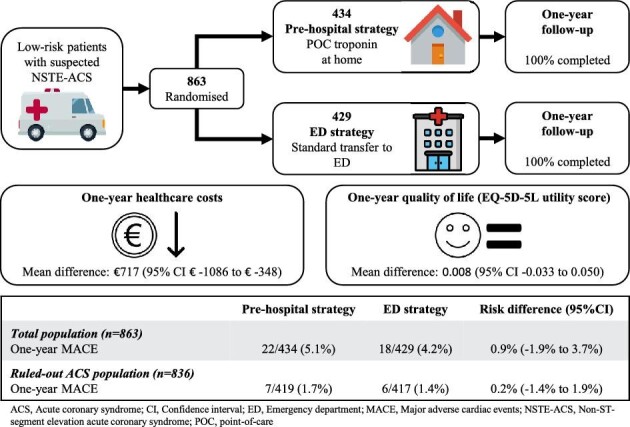
Background and aims: The healthcare burden of acute chest pain is enormous. In the randomized ARTICA trial, we showed that pre-hospital identification of low-risk patients and rule-out of non-ST-segment elevation acute coronary syndrome (NSTE-ACS) with point-of-care (POC) troponin measurement reduces 30-day healthcare costs with low major adverse cardiac events (MACE) incidence. Here we present the final 1-year results of the ARTICA trial.
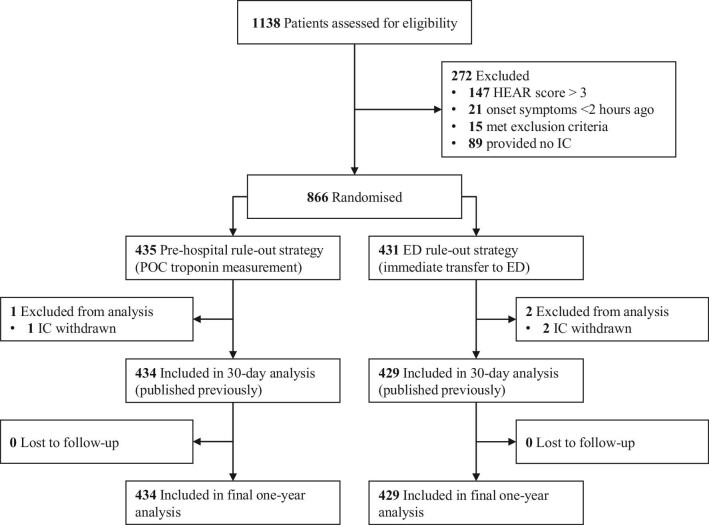
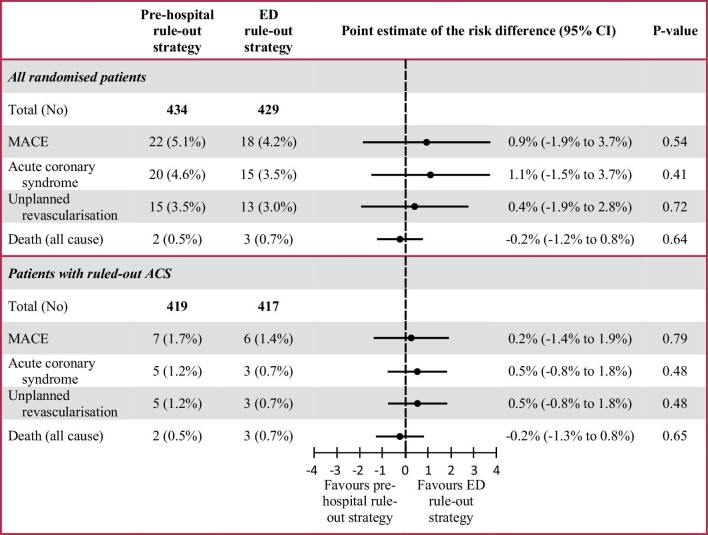
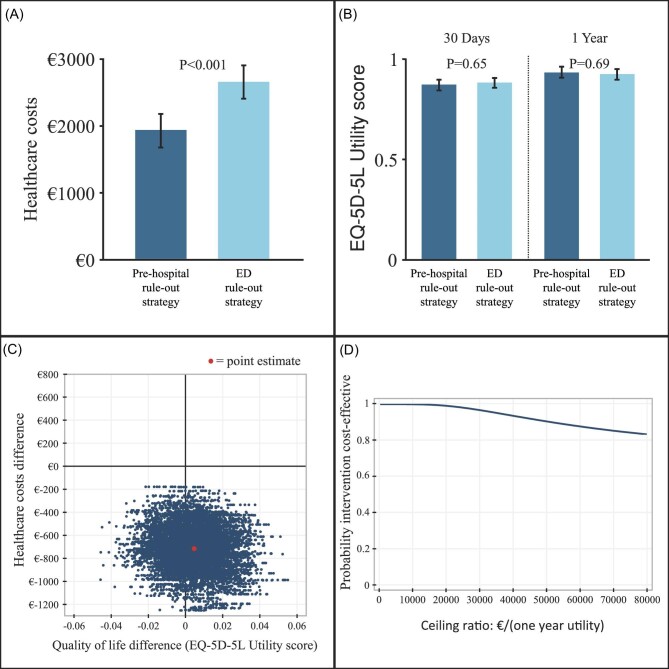
Methods: Low-risk patients with suspected NSTE-ACS were randomized to pre-hospital rule-out with POC troponin measurement or emergency department (ED) transfer. Primary 1-year outcome was healthcare costs. Secondary outcomes were safety, quality of life (QoL), and cost-effectiveness. Safety was defined as a 1-year MACE consisting of ACS, unplanned revascularization, or all-cause death. QoL was measured with EuroQol-5D-5L questionnaires. Cost-effectiveness was defined as 1-year healthcare costs difference per QoL difference.
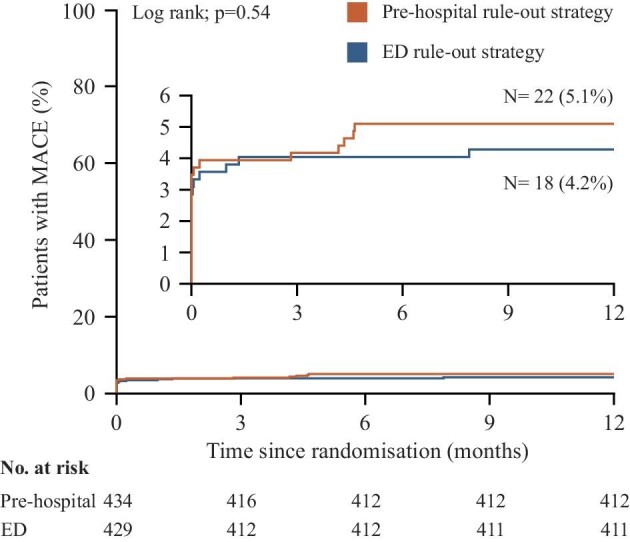
Results: Follow-up was completed for all 863 patients. Healthcare costs were significantly lower in the pre-hospital strategy (€1932 ± €2784 vs. €2649 ± €2750), mean difference €717 [95% confidence interval (CI) €347 to €1087; P < 0.001]. In the total population, the 1-year MACE rate was comparable between groups [5.1% (22/434) in the pre-hospital strategy vs. 4.2% (18/429) in the ED strategy; P = 0.54]. In the ruled-out ACS population, 1-year MACE remained low [1.7% (7/419) vs. 1.4% (6/417)], risk difference 0.2% (95% CI -1.4% to 1.9%; P = 0.79). QoL showed no significant difference between strategies.
Conclusions: Pre-hospital rule-out of NSTE-ACS with POC troponin testing in low-risk patients is cost-effective, as expressed by a sustainable healthcare cost reduction and no significant effect on QoL. One-year MACE remained low for both strategies.
Keywords: Acute coronary syndrome; Ambulance; Cost-effectiveness; Healthcare economics; Point-of-care troponin.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Ambulance drive-thru troponin, ready to go?Eur Heart J Qual Care Clin Outcomes. 2024 Aug 8;10(5):384-385. doi: 10.1093/ehjqcco/qcae023. Eur Heart J Qual Care Clin Outcomes. 2024. PMID: 38692850 No abstract available.
References
-
- Dawson LP, Smith K, Cullen L, Nehme Z, Lefkovits J, Taylor AJet al. . Care models for acute chest pain that improve outcomes and efficiency: JACC state-of-the-art review. J Am Coll Cardiol 2022;79:2333–2348. - PubMed
-
- Collet JP, Thiele H, Barbato E, Barthelemy O, Bauersachs J, Bhatt DLet al. . 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J 2020;41:3495–3497. - PubMed
-
- Writing Committee M, Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DLet al. . 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2021;78:e187–e285. - PubMed
-
- Lee TH, Goldman L. Evaluation of the patient with acute chest pain. N Engl J Med 2000;342:1187–1195. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
