

Triggering receptor expressed on myeloid cells 2 (TREM2) regulates phagocytosis in glioblastoma
- PMID: 38237157
- PMCID: PMC11066944
- DOI: 10.1093/neuonc/noad257
Triggering receptor expressed on myeloid cells 2 (TREM2) regulates phagocytosis in glioblastoma
Abstract
Background: Glioblastomas (GBMs) are central nervous system tumors that resist standard-of-care interventions and even immune checkpoint blockade. Myeloid cells in the tumor microenvironment can contribute to GBM progression; therefore, emerging immunotherapeutic approaches include reprogramming these cells to achieve desirable antitumor activity. Triggering receptor expressed on myeloid cells 2 (TREM2) is a myeloid signaling regulator that has been implicated in a variety of cancers and neurological diseases with contrasting functions, but its role in GBM immunopathology and progression is still under investigation.
Methods: Our reverse translational investigations leveraged single-cell RNA sequencing and cytometry of human gliomas to characterize TREM2 expression across myeloid subpopulations. Using 2 distinct murine glioma models, we examined the role of Trem2 on tumor progression and immune modulation of myeloid cells. Furthermore, we designed a method of tracking phagocytosis of glioma cells in vivo and employed in vitro assays to mechanistically understand the influence of TREM2 signaling on tumor uptake.
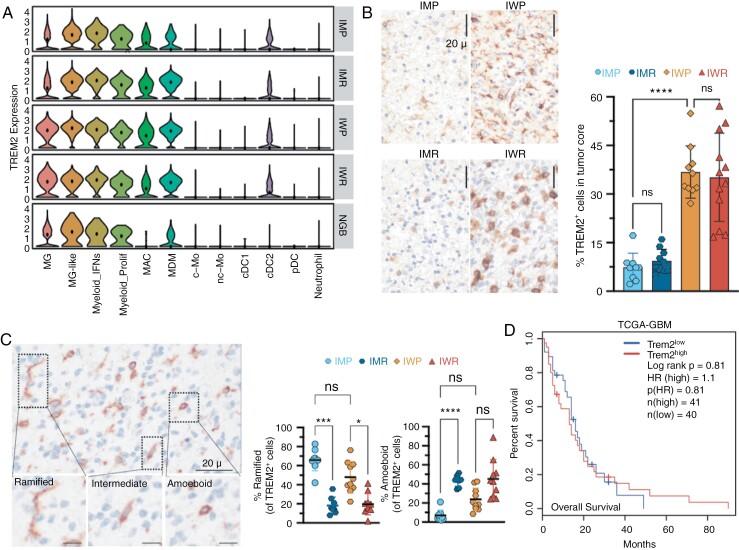
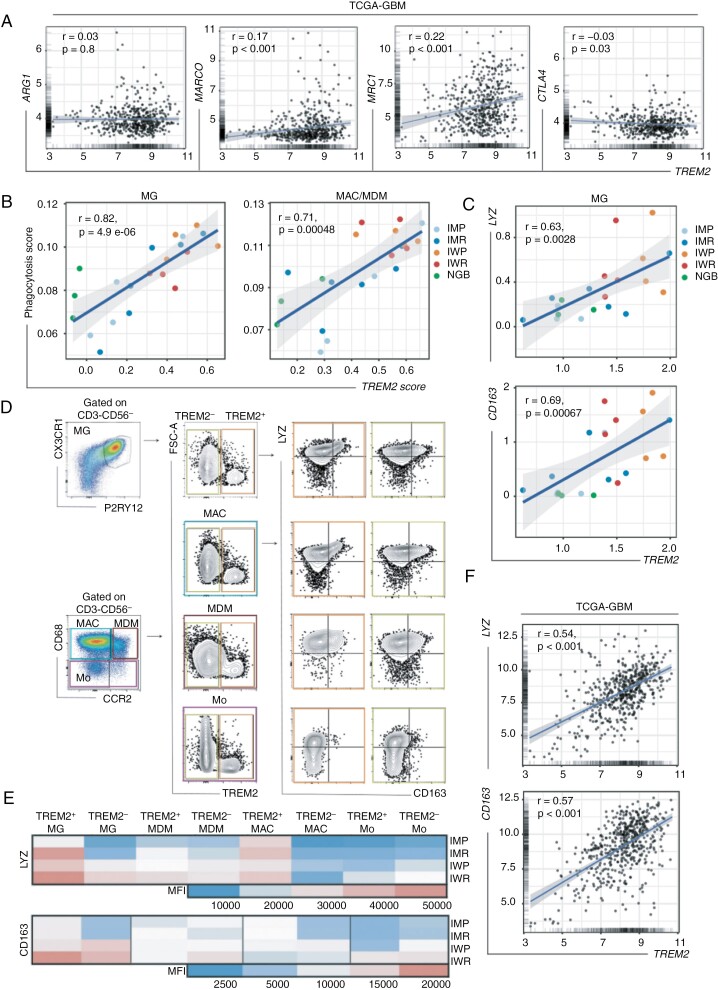
Results: We discovered that TREM2 expression does not correlate with immunosuppressive pathways, but rather showed strong a positive association with the canonical phagocytosis markers lysozyme (LYZ) and macrophage scavenger receptor (CD163) in gliomas. While Trem2 deficiency was found to be dispensable for gliomagenesis, Trem2+ myeloid cells display enhanced tumor uptake compared to Trem2- cells. Mechanistically, we demonstrate that TREM2 mediates phagocytosis via Syk signaling.
Conclusions: These results indicate that TREM2 is not associated with immunosuppression in gliomas. Instead, TREM2 is an important regulator of phagocytosis that may be exploited as a potential therapeutic strategy for brain tumors.
Keywords: TREM2; glioblastoma; microglia; phagocytosis.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Figures



Update of
-
Triggering receptor expressed on myeloid cells 2 (TREM2) regulates phagocytosis in glioblastoma.bioRxiv [Preprint]. 2023 Apr 6:2023.04.05.535792. doi: 10.1101/2023.04.05.535792. bioRxiv. 2023. Update in: Neuro Oncol. 2024 May 3;26(5):826-839. doi: 10.1093/neuonc/noad257. PMID: 37066184 Free PMC article. Updated. Preprint.
Comment in
-
TREM2 function in glioblastoma immune microenvironment: Can we distinguish reality from illusion?Neuro Oncol. 2024 May 3;26(5):840-842. doi: 10.1093/neuonc/noae019. Neuro Oncol. 2024. PMID: 38290471 Free PMC article. No abstract available.
-
TREM2 mediates phagocytosis in glioblastoma.Nat Rev Neurol. 2024 Mar;20(3):133. doi: 10.1038/s41582-024-00935-1. Nat Rev Neurol. 2024. PMID: 38326398 No abstract available.
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Hegi ME, Diserens A-C, Gorlia T, et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med. 2005;352(10):997–1003. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
