

Obesity surgery and neural correlates of human eating behaviour: A systematic review of functional MRI studies
- PMID: 38237270
- PMCID: PMC10828606
- DOI: 10.1016/j.nicl.2024.103563
Obesity surgery and neural correlates of human eating behaviour: A systematic review of functional MRI studies
Abstract
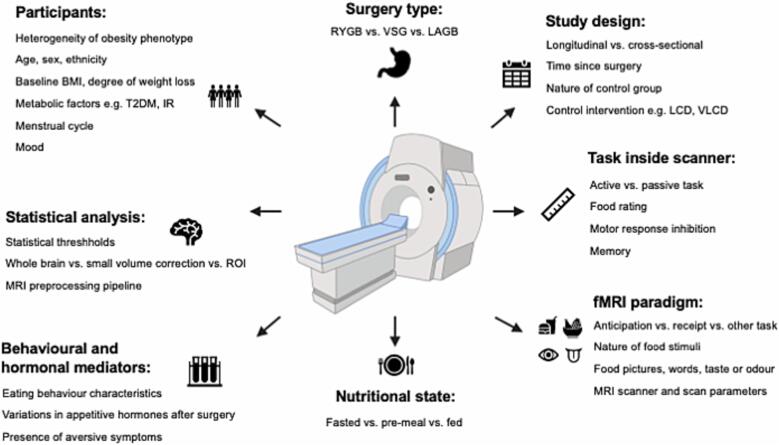
Changes in eating behaviour including reductions in appetite and food intake, and healthier food cue reactivity, reward, hedonics and potentially also preference, contribute to weight loss and its health benefits after obesity surgery. Functional magnetic resonance imaging (fMRI) has been increasingly used to interrogate the neural correlates of eating behaviour in obesity, including brain reward-cognitive systems, changes after obesity surgery, and links with alterations in the gut-hormone-brain axis. Neural responses to food cues can be measured by changes in blood oxygen level dependent (BOLD) signal in brain regions involved in reward processing, including caudate, putamen, nucleus accumbens, insula, amygdala, orbitofrontal cortex, and top-down inhibitory control, including dorsolateral prefrontal cortex (dlPFC). This systematic review aimed to examine: (i) results of human fMRI studies involving obesity surgery, (ii) important methodological differences in study design across studies, and (iii) correlations and associations of fMRI findings with clinical outcomes, other eating behaviour measures and mechanistic measures. Of 741 articles identified, 23 were eligible for inclusion: 16 (69.6%) longitudinal, two (8.7%) predictive, and five (21.7%) cross-sectional studies. Seventeen studies (77.3%) included patients having Roux-en-Y gastric bypass (RYGB) surgery, six (26.1%) vertical sleeve gastrectomy (VSG), and five (21.7%) laparoscopic adjustable gastric banding (LAGB). The majority of studies (86.0%) were identified as having a very low risk of bias, though only six (27.3%) were controlled interventional studies, with none including randomisation to surgical and control interventions. The remaining studies (14.0%) had a low risk of bias driven by their control groups not having an active treatment. After RYGB surgery, food cue reactivity often decreased or was unchanged in brain reward systems, and there were inconsistent findings as to whether reductions in food cue reactivity was greater for high-energy than low-energy foods. There was minimal evidence from studies of VSG and LAGB surgeries for changes in food cue reactivity in brain reward systems, though effects of VSG surgery on food cue reactivity in the dlPFC were more consistently found. There was consistent evidence for post-operative increases in satiety gut hormones glucagon-like-peptide 1 (GLP-1) and peptide YY (PYY) mediating reduced food cue reactivity after RYGB surgery, including two interventional studies. Methodological heterogeneity across studies, including nutritional state, nature of food cues, post-operative timing, lack of control groups for order effects and weight loss or dietary/psychological advice, and often small sample sizes, limited the conclusions that could be drawn, especially for correlational analyses with clinical outcomes, other eating behaviour measures and potential mediators. This systematic review provides a detailed data resource for those performing or analysing fMRI studies of obesity surgery and makes suggestions to help improve reporting and design of such studies, as well as future directions.
Keywords: Appetite; Bariatric surgery; Food; Gastric bypass; Sleeve gastrectomy; fMRI.
Copyright © 2024. Published by Elsevier Inc.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




References
-
- Adams T.D., Davidson L.E., Hunt S.C. Weight and Metabolic Outcomes 12 Years after Gastric Bypass. N. Engl. J. Med. 2018;378:93–96. - PubMed
-
- Al-Alsheikh A.S., Alabdulkader S., Miras A.D., Goldstone A.P. Effects of Bariatric Surgery and Dietary Interventions for Obesity on Brain Neurotransmitter Systems and Metabolism: a Systematic Review of Positron Emission Tomography (PET) and Single-Photon Emission Computed Tomography (SPECT) Studies. Obes. Rev. 2023;24:e13620. - PMC - PubMed
-
- Al-Najim W., Docherty N.G., le Roux C.W. Food Intake and Eating Behavior After Bariatric Surgery. Physiol. Rev. 2018;98:1113–1141. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
