

Diffusion-Weighted Imaging Reveals Impaired Glymphatic Clearance in Idiopathic Intracranial Hypertension
- PMID: 38238097
- PMCID: PMC11285988
- DOI: 10.3174/ajnr.A8088
Diffusion-Weighted Imaging Reveals Impaired Glymphatic Clearance in Idiopathic Intracranial Hypertension
Abstract
Background and purpose: The pathophysiology underlying idiopathic intracranial hypertension (IIH) remains incompletely understood. While one theory postulates impaired cerebral glymphatic clearance in IIH, there is a paucity of methods to quantify glymphatic activity in human brains. The purpose of this study was to use advanced diffusion-weighed imaging to evaluate the glymphatic clearance of IIH patients and how it may relate to clinical severity.
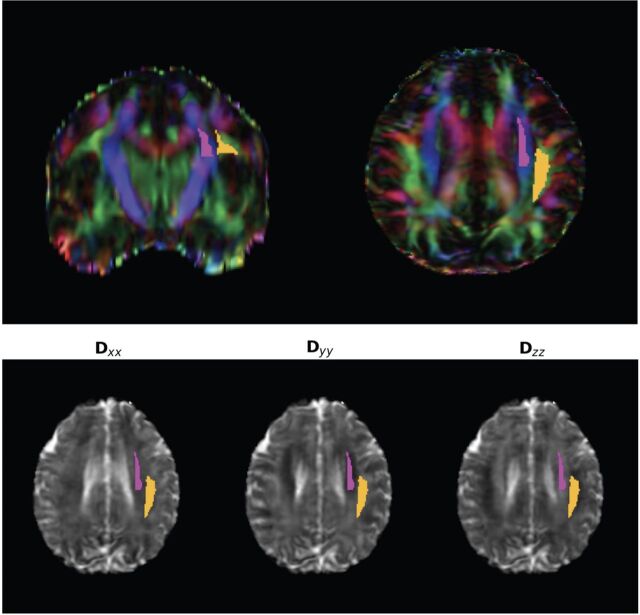
Materials and methods: DWI was used to separately evaluate the diffusivity along the cerebral perivascular spaces and lateral association and projection fibers, with the degree of diffusivity used as a surrogate for glymphatic function (diffusion tensor image analysis along the perivascular space. Patients with IIH were compared with normal controls. Glymphatic clearance was correlated with several clinical metrics, including lumbar puncture opening pressure and Frisen papilledema grade (low grade: 0-2; high grade: 3-5).
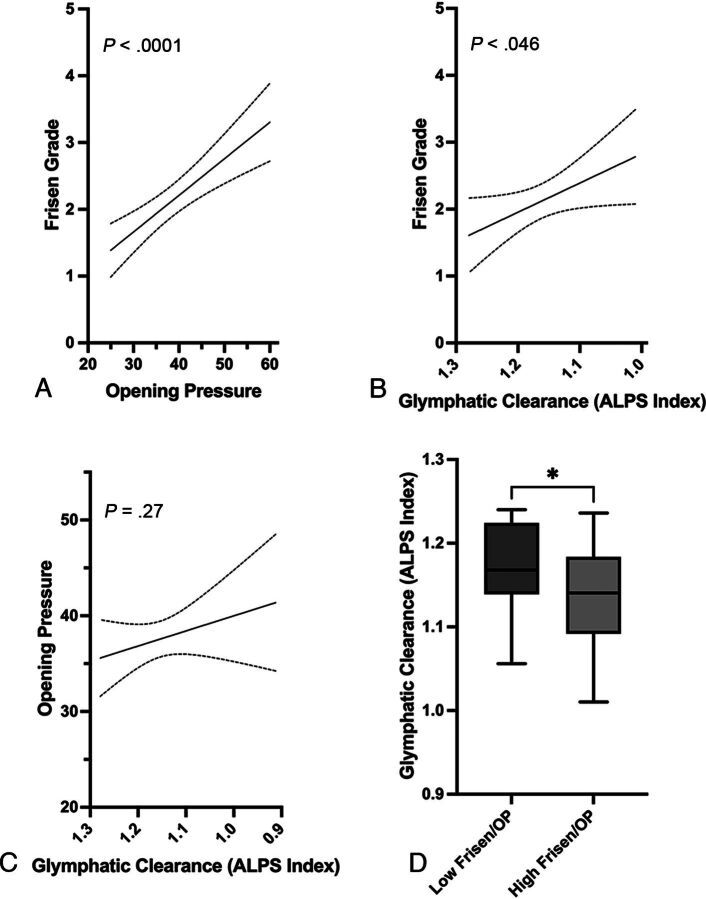
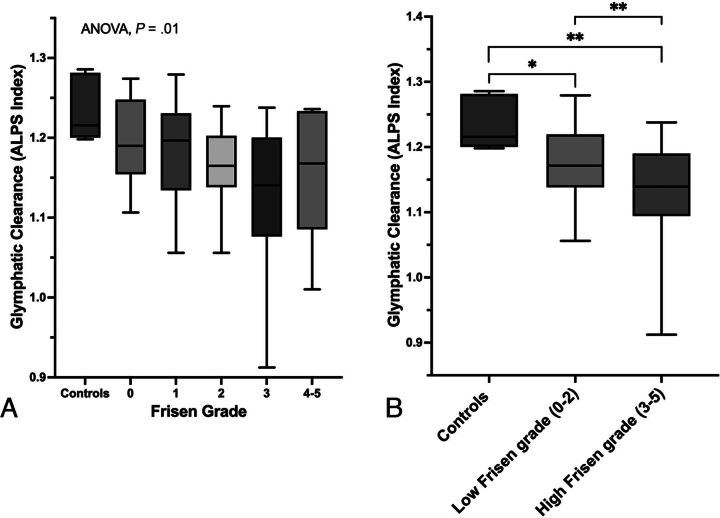
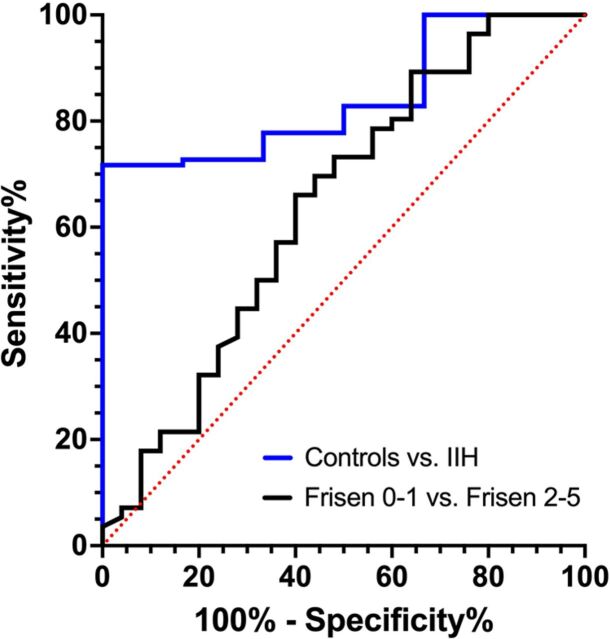
Results: In total, 99 patients with IIH were identified and compared with 6 healthy controls. Overall, patients with IIH had significantly lower glymphatic clearance based on DWI-derived diffusivity compared with controls (P = .005). Additionally, in patients with IIH, there was a significant association between declining glymphatic clearance and increasing Frisen papilledema grade (P = .046) but no correlation between opening pressure and glymphatic clearance (P = .27). Furthermore, healthy controls had significantly higher glymphatic clearance compared with patients with IIH and low-grade papilledema (P = .015) and high-grade papilledema (P = .002). Lastly, patients with IIH and high-grade papilledema had lower glymphatic clearance compared with patients with IIH and low-grade papilledema (P = .005).
Conclusions: Patients with IIH possess impaired glymphatic clearance, which is directly related to the extent of clinical severity. The DWI-derived parameters can be used for clinical diagnosis or to assess response to treatment.
© 2024 by American Journal of Neuroradiology.
Figures
Similar articles
-
Optic Nerve Sheath Dilation Is a Possible Marker of CSF Dyshomeostasis in Idiopathic Intracranial Hypertension.Clin Neuroradiol. 2025 Jun;35(2):239-245. doi: 10.1007/s00062-024-01476-2. Epub 2024 Nov 25. Clin Neuroradiol. 2025. PMID: 39585390
-
Association of Extent of Transverse Sinus Stenosis With Cerebral Glymphatic Clearance in Patients With Idiopathic Intracranial Hypertension.Neurology. 2024 Jul 9;103(1):e209529. doi: 10.1212/WNL.0000000000209529. Epub 2024 Jun 4. Neurology. 2024. PMID: 38833652
-
Increased brain volume in idiopathic intracranial hypertension: Association with intracranial pressure and papilledema severity.J Neurol Sci. 2025 Jun 15;473:123501. doi: 10.1016/j.jns.2025.123501. Epub 2025 Apr 12. J Neurol Sci. 2025. PMID: 40239382
-
Role of the glymphatic system in idiopathic intracranial hypertension.Clin Neurol Neurosurg. 2022 Nov;222:107446. doi: 10.1016/j.clineuro.2022.107446. Epub 2022 Sep 17. Clin Neurol Neurosurg. 2022. PMID: 36183631 Review.
-
The Role of Arachnoid Granulations and the Glymphatic System in the Pathophysiology of Idiopathic Intracranial Hypertension.Curr Neurol Neurosci Rep. 2020 May 22;20(7):20. doi: 10.1007/s11910-020-01044-4. Curr Neurol Neurosci Rep. 2020. PMID: 32444998 Review.
Cited by
-
Regulation of brain fluid volumes and pressures: basic principles, intracranial hypertension, ventriculomegaly and hydrocephalus.Fluids Barriers CNS. 2024 Jul 17;21(1):57. doi: 10.1186/s12987-024-00532-w. Fluids Barriers CNS. 2024. PMID: 39020364 Free PMC article. Review.
-
Rare Complications of CSF Diversion: Paradoxical Neuroimaging Findings in a Double, Chiasmic Case Report.Diagnostics (Basel). 2024 May 30;14(11):1141. doi: 10.3390/diagnostics14111141. Diagnostics (Basel). 2024. PMID: 38893666 Free PMC article.
-
Optic Nerve Sheath Dilation Is a Possible Marker of CSF Dyshomeostasis in Idiopathic Intracranial Hypertension.Clin Neuroradiol. 2025 Jun;35(2):239-245. doi: 10.1007/s00062-024-01476-2. Epub 2024 Nov 25. Clin Neuroradiol. 2025. PMID: 39585390
-
Improved Cerebral Glymphatic Flow after Transvenous Embolization of CSF-Venous Fistula.AJNR Am J Neuroradiol. 2024 Jul 8;45(7):961-964. doi: 10.3174/ajnr.A8229. AJNR Am J Neuroradiol. 2024. PMID: 38697791 Free PMC article.
-
The Glymphatic System and Its Role in Neurovascular Diseases.J Neuroendovasc Ther. 2025;19(1):2025-0020. doi: 10.5797/jnet.ra.2025-0020. Epub 2025 Jun 21. J Neuroendovasc Ther. 2025. PMID: 40548139 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources