

Dynamic Anterior Stabilization with Hill-Sachs Remplissage Can be Employed in Skeletally Immature Patients-Operative Technique
- PMID: 38238248
- PMCID: PMC10925509
- DOI: 10.1111/os.13989
Dynamic Anterior Stabilization with Hill-Sachs Remplissage Can be Employed in Skeletally Immature Patients-Operative Technique
Abstract
Background: Numerous studies indicate that glenoid bony augmentation raises the risk of complications during and after surgery. On the other hand, repairing the labrum alone in cases with subcritical glenoid bone loss results in recurrent instability and persistent apprehension. As a result, recent advancements in shoulder instability surgery prioritize fully restoring the anterior shoulder restraint.
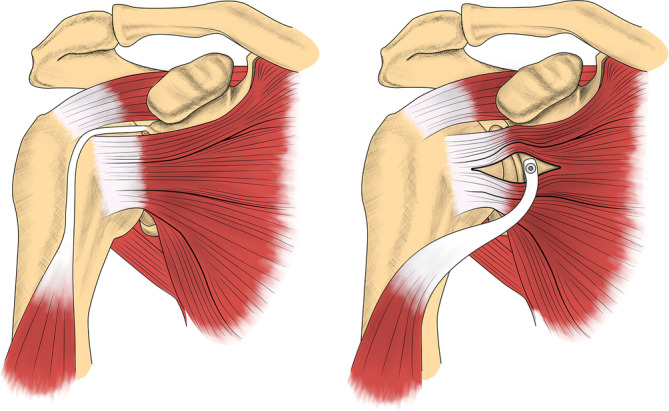
Operative technique: A novel method for treating recurrent anterior shoulder instability with subcritical glenoid bone loss and off-track Hill-Sachs lesion in skeletally immature patients is suggested: the use of dynamic anterior stabilization technique incorporating the long head of the biceps tendon onto the anterior glenoid rim via trans-subscapular transfer, in conjunction with Hill-Sachs remplissage. A practical, step-by-step surgical technique for a complete reconstruction of the anterior capsule-labral-ligamentous complex is provided. This involves utilizing a soft-tissue dynamic anterior sling, achieved through the trans-subscapularis transfer of the long head of the biceps tendon at the glenoid level. The procedure concludes with a Hill-Sachs remplissage to further prevent off-track events and alleviate apprehension.
Conclusion: Dynamic anterior stabilization is a suitable approach for addressing recurring anterior shoulder instability in skeletally immature patients who have subcritical glenoid bone loss and bipolar bone lesions.
Keywords: Anterior shoulder instability; Bankart repair; Complications in shoulder instability procedures; Dynamic anterior stabilization; Glenoid bone loss; Remplissage.
© 2024 The Authors. Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare that they have no conflict of interests related to the subject of the article. They have not received or will receive any financial aid, in any form, for this study. The manuscript has been prepared according to the journal's style specifications and requirements.
Figures


Similar articles
-
Remplissage Versus Modified Latarjet for Off-Track Hill-Sachs Lesions With Subcritical Glenoid Bone Loss.Am J Sports Med. 2018 Jul;46(8):1885-1891. doi: 10.1177/0363546518767850. Epub 2018 Apr 19. Am J Sports Med. 2018. PMID: 29672132
-
Remplissage for Anterior Shoulder Instability: History, Indications, and Outcomes.Orthop Clin North Am. 2022 Jul;53(3):327-338. doi: 10.1016/j.ocl.2022.02.005. Epub 2022 May 27. Orthop Clin North Am. 2022. PMID: 35725041 Review.
-
Arthroscopic Bankart Repair With Remplissage in Comparison to Bone Block Augmentation for Anterior Shoulder Instability With Bipolar Bone Loss: A Systematic Review.Arthroscopy. 2021 Feb;37(2):706-717. doi: 10.1016/j.arthro.2020.08.033. Epub 2020 Sep 7. Arthroscopy. 2021. PMID: 32911004
-
Additional Scapular Spine Bone Grafting Combined with Bankart and Remplissage for Off-Track Hill-Sachs Lesions with Subcritical Glenoid Bone Loss: Provides Better Stability.Orthop Surg. 2024 Nov;16(11):2644-2653. doi: 10.1111/os.14158. Epub 2024 Sep 23. Orthop Surg. 2024. PMID: 39312469 Free PMC article.
-
Editorial Commentary: For Patients With Shoulder Instability, On-Track Hill-Sachs Lesion Plus Subcritical Glenoid Bone Loss May Be the Best Indication for Dynamic Anterior Stabilization Using the Long Head of the Biceps Tendon.Arthroscopy. 2024 Jul;40(7):1994-1996. doi: 10.1016/j.arthro.2024.02.030. Epub 2024 Mar 4. Arthroscopy. 2024. PMID: 38447627
Cited by
-
Research on the application effect of arthroscopic access modification in meniscal injury repair.J Orthop Surg Res. 2025 Jan 3;20(1):5. doi: 10.1186/s13018-024-05434-z. J Orthop Surg Res. 2025. PMID: 39754209 Free PMC article.
-
Arthroscopic Parallel Double-Pulley Iliac Crest Bone Graft Fixation for Anterior Glenoid Reconstruction.Arthrosc Tech. 2024 Dec 25;14(5):103401. doi: 10.1016/j.eats.2024.103401. eCollection 2025 May. Arthrosc Tech. 2024. PMID: 40548019 Free PMC article.
-
Ultrasound-Based Anatomical Assessment of the Most Common Shoulder Soft Tissue Injuries in Young Adults.Healthcare (Basel). 2025 Aug 13;13(16):1984. doi: 10.3390/healthcare13161984. Healthcare (Basel). 2025. PMID: 40868600 Free PMC article.
-
The Evolution of Arthroscopic Shoulder Surgery: Current Trends and Future Perspectives.J Clin Med. 2025 Apr 1;14(7):2405. doi: 10.3390/jcm14072405. J Clin Med. 2025. PMID: 40217855 Free PMC article. Review.
-
Dynamic anterior stabilization for recurrent anterior shoulder instability improves postoperative patient-reported outcomes without restricting shoulder range of motion: a meta-analysis.Int Orthop. 2025 Aug;49(8):1931-1941. doi: 10.1007/s00264-025-06581-6. Epub 2025 Jun 16. Int Orthop. 2025. PMID: 40522491
References
-
- Bah A, Lateur GM, Kouevidjin BT, Bassinga JYS, Issa M, Jaafar A, et al. Chronic anterior shoulder instability with significant Hill–Sachs lesion: arthroscopic Bankart with remplissage versus open Latarjet procedure. Orthop Traumatol Surg Res. 2018;104(1):17–22. 10.1016/j.otsr.2017.11.009 - DOI - PubMed
-
- Franklin CC, Weiss JM. The natural history of pediatric and adolescent shoulder dislocation. J Pediatr Orthop. 2019;39:S50–S52. - PubMed
-
- Camus D, Domos P, Berard E, Toulemonde J, Mansat P, Bonnevialle N. Isolated arthroscopic Bankart repair vs. Bankart repair with “remplissage” for anterior shoulder instability with engaging Hill‐Sachs lesion: a meta‐analysis. Orthop Traumatol Surg Res. 2018;104(6):803–809. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
