

Exploring potential causal associations between autoimmune diseases and colorectal cancer using bidirectional Mendelian randomization
- PMID: 38238429
- PMCID: PMC10796354
- DOI: 10.1038/s41598-024-51903-0
Exploring potential causal associations between autoimmune diseases and colorectal cancer using bidirectional Mendelian randomization
Abstract
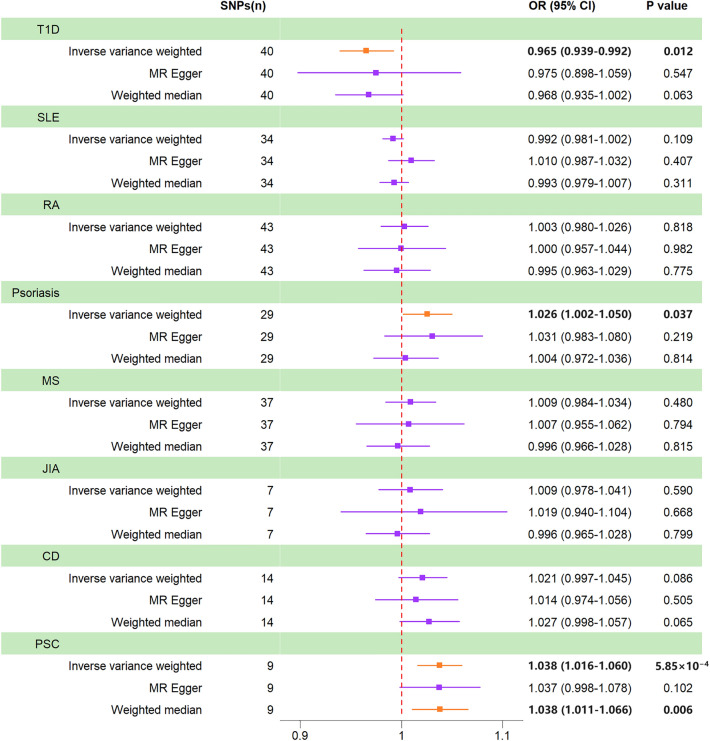
Several observational studies have revealed an association between autoimmune diseases (AIDs) and colorectal cancer (CRC), although their causal association remained controversial. Therefore, our study used a two-sample Mendelian randomization (MR) analysis to verify the causal association between AIDs and CRC. We employed three common MR approaches, including inverse variance weighted (IVW), weighted median, and MR-Egger methods, to assess the causal association between type 1 diabetes (T1D), systemic lupus erythematosus, rheumatoid arthritis, psoriasis, multiple sclerosis, juvenile idiopathic arthritis, celiac disease, and primary sclerosing cholangitis (PSC) and CRC. The reverse MR analysis was performed to assess the possibility of reverse causation. To evaluate the validity of the analysis, we also performed sensitivity analysis, such as the heterogeneity test, the horizontal pleiotropy test, and the leave-one-out sensitivity analysis, and validated the results in the validation cohort. Our results showed that genetically predicted T1D was nominally associated with a lower risk of CRC (IVW OR = 0.965, 95% CI = 0.939-0.992, P = 0.012). However, genetic susceptibility to psoriasis nominally increased the risk of CRC (IVW OR = 1.026, 95% CI = 1.002-1.050, P = 0.037). Genetically predicted PSC had a significant causal effect on the increasing risk of CRC (IVW OR = 1.038, 95% CI = 1.016-1.060, P = 5.85 × 10-4). Furthermore, the MR analysis between PSC and the CRC validation cohort indicated consistent results. We found no causal association between genetically predicted other five AIDs and CRC (P > 0.05). The results of reverse MR analysis showed that genetically predicted CRC had no causal effect on T1D, psoriasis, and PSC (P > 0.05). The sensitivity analysis demonstrated that the results of the MR analysis were reliable. Our findings help to understand the causal association between AIDs and CRC, which deserves further investigation.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Causal associations between liver traits and Colorectal cancer: a Mendelian randomization study.BMC Med Genomics. 2023 Dec 6;16(1):316. doi: 10.1186/s12920-023-01755-w. BMC Med Genomics. 2023. PMID: 38057864 Free PMC article.
-
Investigation of the causal association between Parkinson's disease and autoimmune disorders: a bidirectional Mendelian randomization study.Front Immunol. 2024 May 7;15:1370831. doi: 10.3389/fimmu.2024.1370831. eCollection 2024. Front Immunol. 2024. PMID: 38774879 Free PMC article.
-
Genetic link between primary sclerosing cholangitis and thyroid dysfunction: a bidirectional two-sample Mendelian randomization study.Front Immunol. 2023 Oct 19;14:1276459. doi: 10.3389/fimmu.2023.1276459. eCollection 2023. Front Immunol. 2023. PMID: 37928559 Free PMC article.
-
Association between Omega-3 fatty acids and autoimmune disease: Evidence from the umbrella review and Mendelian randomization analysis.Autoimmun Rev. 2024 Nov;23(11):103651. doi: 10.1016/j.autrev.2024.103651. Epub 2024 Sep 30. Autoimmun Rev. 2024. PMID: 39357585 Review.
-
Application of Mendelian randomization analysis in investigating the genetic background of blood biomarkers for colorectal cancer.Yi Chuan. 2024 Oct;46(10):833-848. doi: 10.16288/j.yczz.24-179. Yi Chuan. 2024. PMID: 39443312 Review.
Cited by
-
Study on the causality of cathepsin on autoimmune diseases and cancer: evidence from mendelian randomization analysis.Arch Dermatol Res. 2024 Dec 14;317(1):125. doi: 10.1007/s00403-024-03607-8. Arch Dermatol Res. 2024. PMID: 39673556
-
Type I Diabetes Mellitus impairs cytotoxic immunity through CEACAM5 upregulation in colorectal cancer : Exploring the intersection of autoimmune dysfunction and cancer progression: the role of NF-κB p65 in colorectal cancer.J Mol Histol. 2024 Dec;55(6):1285-1293. doi: 10.1007/s10735-024-10269-3. Epub 2024 Oct 18. J Mol Histol. 2024. PMID: 39419943
-
Genetic insights into the shared molecular mechanisms of Crohn's disease and breast cancer: a Mendelian randomization and deep learning approach.Discov Oncol. 2025 Feb 18;16(1):198. doi: 10.1007/s12672-025-01978-6. Discov Oncol. 2025. PMID: 39964572 Free PMC article.
-
Immune cells mediate the causal relationship between uveitis and colorectal cancer via Mendelian randomization analysis.Sci Rep. 2024 Oct 29;14(1):25964. doi: 10.1038/s41598-024-77758-z. Sci Rep. 2024. PMID: 39472473 Free PMC article.
-
Investigating the Causality and Pathogenesis of Primary Sclerosing Cholangitis in Colorectal Cancer Through Mendelian Randomization and Bioinformatics.Genet Res (Camb). 2025 May 18;2025:5887056. doi: 10.1155/genr/5887056. eCollection 2025. Genet Res (Camb). 2025. PMID: 40432804 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
